
Dr. Alessandro Giardini
If you have been told that your child has pulmonary valve stenosis, it is completely natural to feel concerned. The reassuring news is that pulmonary valve stenosis is one of the most common congenital heart defects, accounting for approximately 8 to 10% of all cardiac birth defects, and the outlook for children with this condition is excellent. Many children with mild stenosis need no treatment at all, and when intervention is required, balloon valvuloplasty is highly effective and avoids the need for open-heart surgery in the vast majority of cases.
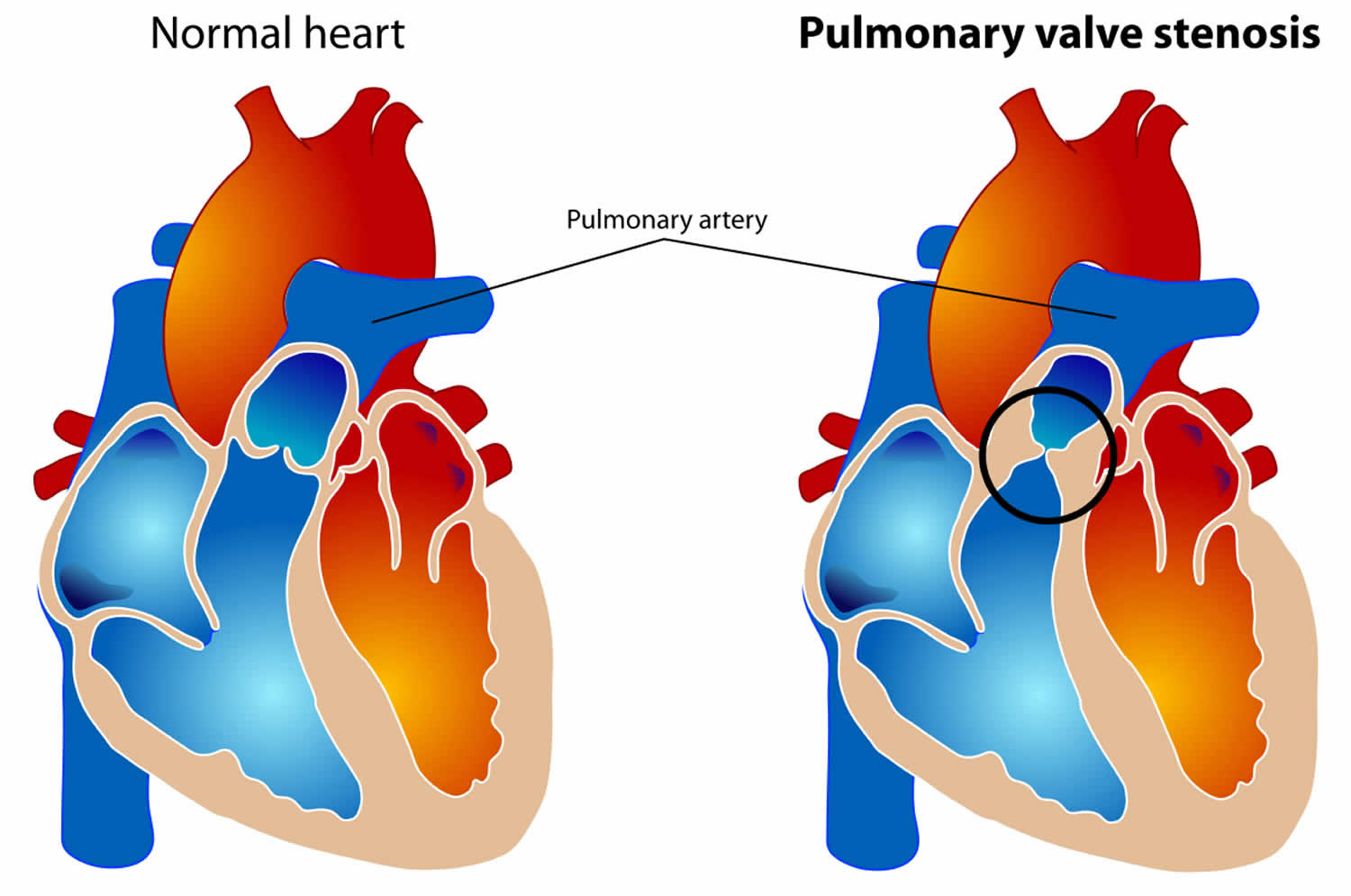
The pulmonary valve sits between the right ventricle (the heart's right-sided pumping chamber) and the pulmonary artery, which carries blood to the lungs to pick up oxygen. In a normal heart, this valve opens fully with each heartbeat to allow blood to flow freely into the lungs, and closes between beats to prevent blood from leaking back into the right ventricle.
In pulmonary valve stenosis, the valve leaflets are thickened, stiffened or fused together and do not open fully. This creates a narrowing that obstructs the flow of blood from the right ventricle to the lungs, forcing the heart to work harder to push blood through the restricted opening. Over time, this extra workload causes the muscular wall of the right ventricle to thicken, a response known as right ventricular hypertrophy. If the stenosis is severe and left untreated, the right ventricle may eventually tire and its pumping function may weaken.
The severity of pulmonary valve stenosis is classified according to the pressure difference (gradient) measured across the valve on echocardiography. A gradient below 40 mmHg is considered mild, between 40 and 60 mmHg is moderate, and above 60 mmHg is severe. This classification is important because it guides decisions about whether monitoring alone is sufficient or whether treatment is needed.
It is worth noting that narrowing of the right ventricular outflow tract can also occur at levels other than the valve itself. Subvalvular (infundibular) stenosis involves thickened muscle below the valve, while supravalvular stenosis affects the pulmonary artery above the valve. These are distinct conditions with different implications, and Dr Giardini will clarify exactly where the narrowing is located during the echocardiographic assessment.
The exact cause is not known in most children. The valve simply forms abnormally during the early weeks of pregnancy, and in the vast majority of cases nothing a parent did or did not do played any role.
In some children, pulmonary valve stenosis is associated with genetic syndromes. Noonan syndrome is the most well-recognised association. Children with Noonan syndrome often have a distinctive form of pulmonary stenosis in which the valve leaflets are thick, fleshy and immobile rather than simply fused. This is known as a dysplastic pulmonary valve, and it is important to identify because dysplastic valves tend to respond less well to balloon valvuloplasty than the more common fused (dome-shaped) variety. Williams syndrome and certain infections acquired in the womb, such as rubella, can also cause pulmonary stenosis. In some children, pulmonary valve stenosis occurs alongside other congenital heart defects rather than in isolation.
Children with mild pulmonary valve stenosis have no symptoms at all. They grow and develop normally, are fully active, and the condition is typically discovered only because a doctor hears a heart murmur during a routine examination.
Children with moderate degrees of stenosis may remain well for a long time, but some develop symptoms during intense physical exertion. These may include breathlessness, increased fatigue, or a feeling of reduced stamina compared to their peers. It is important to be aware that in young children, particularly during the first year of life, moderate stenosis can sometimes progress and become more severe as the valve fails to grow in proportion with the child.
Children with severe pulmonary valve stenosis usually have more noticeable symptoms. These may include chest pain during exercise, tiredness, palpitations and reduced exercise tolerance. When the stenosis is very severe, symptoms can occur even at rest. In babies with critical pulmonary stenosis, a blue discolouration of the skin, lips and fingernails (cyanosis) may appear because not enough blood is reaching the lungs and oxygen-poor blood is being diverted into the body's circulation through the foramen ovale.
Critical pulmonary stenosis in a newborn is a medical emergency. In this situation, the baby depends on the ductus arteriosus (a normal fetal blood vessel) to maintain blood flow to the lungs. When this vessel begins to close naturally after birth, oxygen levels drop. An intravenous infusion of prostaglandin E1 (alprostadil) is given urgently to keep the ductus open as a life-saving bridge while definitive treatment is arranged.
🟢 GREEN – Usually reassuring
Continue routine follow-up with your paediatric cardiologist
🟡 AMBER – Needs specialist review
Arrange a paediatric cardiology review
🔴 RED – Needs urgent assessment
Seek urgent medical review immediately
In children with mild degrees of pulmonary stenosis, it is a common occurrence that the stenosis improves over time. This is reassuring and is one of the reasons why many children with mild narrowing are simply monitored. However, even children with mild pulmonary stenosis require lifelong follow-up, because the pulmonary valve may become stiffer and work less efficiently later in life as the valve tissue gradually calcifies or fibroses with age. Dr Giardini will explain what this means for your child's individual follow-up schedule.
Most cases are first suspected when a doctor hears a heart murmur during a clinical examination. The murmur of pulmonary valve stenosis is typically a harsh, ejection-type sound heard best at the upper left side of the chest.
The key diagnostic test is an echocardiogram, a painless ultrasound scan of the heart. Dr Giardini performs and interprets all echocardiograms personally, allowing the valve anatomy to be visualised directly, the severity of the narrowing measured accurately using the pressure gradient, the thickness and function of the right ventricle assessed, and any associated heart defects identified. Results are available immediately and can be discussed during the same appointment.
An electrocardiogram (ECG) is also frequently performed to check for signs of right ventricular thickening. In some children, particularly those with unusual anatomy or when the narrowing extends beyond the valve into the pulmonary arteries, a cardiac MRI or chest CT may be recommended to define the anatomy in greater detail and help plan treatment.
Not always. Children with mild and many with moderate degrees of stenosis require only ongoing monitoring with regular clinical appointments and echocardiography. As long as the gradient remains stable, the right ventricle is coping well and the child has no symptoms, no intervention is needed.
Treatment is recommended for children with severe pulmonary stenosis, because the sustained extra workload will ultimately affect the right ventricle, and delaying treatment until the ventricle is already struggling makes any procedure more risky. Treatment is also considered when moderate stenosis is progressing, when symptoms are present, or when there is clear evidence of significant right ventricular thickening on echocardiography.
The great majority of children and adolescents with pulmonary valve stenosis can be treated with a keyhole procedure called balloon valvuloplasty, which is now established as the treatment of choice for this condition.
Balloon valvuloplasty is performed in a catheterisation laboratory under general anaesthetic. A thin, flexible tube (catheter) with a deflated balloon at its tip is inserted through a vein in the leg and advanced through the heart to the pulmonary valve. The balloon is then positioned across the narrowed valve and inflated briefly, forcefully stretching the fused leaflets apart and widening the opening. The balloon is then deflated and the catheter removed. The entire procedure typically takes about an hour. You can see how balloon valvuloplasty works in the video below.
Published long-term follow-up studies confirm that balloon valvuloplasty achieves excellent results, with success rates of approximately 88 to 92% in children with typical valvular stenosis. The pressure gradient across the valve drops significantly immediately after the procedure and continues to improve further during follow-up. Re-stenosis requiring a second procedure occurs in fewer than 5% of cases.
It is important for parents to understand that although the procedure is very effective at relieving the narrowing, it does not make the pulmonary valve completely normal. The valvuloplasty may cause a degree of pulmonary valve leakage (regurgitation), which in most children is mild and very well tolerated. Published data show that this mild regurgitation does not tend to progress significantly over time. However, in a small number of patients, the regurgitation can become more significant over the years and may eventually require consideration of pulmonary valve replacement, typically in adolescence or adulthood. This is one of the reasons why lifelong follow-up remains important.
Surgical treatment may be needed if balloon valvuloplasty is not effective, if the valve is too small or dysplastic to respond to balloon dilatation, or if there are associated heart defects that require surgical correction at the same time. Surgical valvotomy or valve repair through open-heart surgery is safe and effective, and outcomes are excellent.
Children with pulmonary valve stenosis have a small risk of developing endocarditis, an infection of the heart valve caused by bacteria entering the bloodstream. Good dental hygiene, including regular brushing, flossing and routine dental visits, is the most important way to reduce this risk. Current guidelines do not recommend routine antibiotics before dental procedures for most children with pulmonary valve stenosis, although this may be advised for the first six months after any valve intervention. Dr Giardini will advise on whether specific endocarditis precautions apply to your child.
Children with mild pulmonary valve stenosis and many with moderate stenosis can undertake any type of physical activity, including competitive sport, without restriction. Dr Giardini has particular expertise in sport cardiology and can provide individualised exercise guidance based on your child's specific findings.
Children with significant pulmonary valve stenosis may need some activity restriction depending on the severity of the gradient, the function of the right ventricle and the presence of symptoms. In general, moderate-intensity recreational activity remains appropriate for most children, while very high-intensity competitive sport or heavy isometric exercise may be restricted until the stenosis is treated. After successful balloon valvuloplasty, the large majority of children can return to full, unrestricted physical activity.
The long-term outlook for children with pulmonary valve stenosis is excellent, whether they have been managed with monitoring alone, balloon valvuloplasty or surgical treatment. No long-term medications are required. The right ventricle typically recovers well after successful relief of the obstruction, and most children go on to lead completely normal, active lives.
A very small number of children may require further procedures later in life, either for re-stenosis or for progressive pulmonary regurgitation. Modern transcatheter pulmonary valve replacement techniques mean that even when a second intervention is needed, it can often be performed without open-heart surgery.
Children with treated pulmonary valve stenosis require regular ongoing follow-up with a paediatric cardiologist, and this continues into adult life through transition to an adult congenital heart disease service. If you have any concerns about your child or would like to arrange an assessment, please do not hesitate to contact Dr Giardini's team to book an appointment.
In most cases, no. Mild stenosis is harmless and often improves on its own. Moderate and severe stenosis can place strain on the heart if untreated, but with appropriate treatment the outcomes are excellent.
Yes. In children with mild stenosis, the gradient frequently improves over time. However, even when the stenosis is mild, lifelong follow-up is recommended because the valve may become stiffer with age.
The large majority of children who need treatment are treated with balloon valvuloplasty, a keyhole procedure that avoids open-heart surgery entirely. Surgery is only needed in a small number of cases where the valve anatomy is not suitable for balloon treatment.
A catheter with a balloon at its tip is inserted through a vein in the leg and guided to the narrowed pulmonary valve. The balloon is inflated briefly to stretch the valve open. The procedure takes about an hour, is performed under general anaesthetic, and most children go home within a day or two.
The procedure is very safe, with success rates above 88% and a very low complication rate. The most common consequence is mild leakage of the pulmonary valve, which is usually well tolerated and does not progress significantly over time.
Children with mild or successfully treated stenosis can participate fully in sport and physical activity with no restrictions. Those with significant untreated stenosis may need some activity guidance until treatment is performed. Dr Giardini provides individualised sport advice for each child.
A dysplastic valve has thick, immobile leaflets rather than fused ones. It is more commonly seen in children with Noonan syndrome and tends to respond less well to balloon valvuloplasty, sometimes requiring surgical treatment instead.
This is a severe form of stenosis seen in newborn babies where very little blood can pass through the valve. It is a medical emergency requiring urgent treatment, usually with prostaglandin medication to maintain blood flow to the lungs followed by balloon valvuloplasty.
In most cases, routine antibiotic prophylaxis is not required. It may be recommended for the first six months after valve treatment. Good dental hygiene is the most effective way to prevent endocarditis.
Children with pulmonary valve stenosis need regular follow-up with echocardiography, typically every one to two years depending on the severity. This monitoring continues into adulthood to check for any late changes in valve function.
Author: Dr. Alessandro Giardini, MD, PhD
Written 03/04/2026