
Dr. Alessandro Giardini
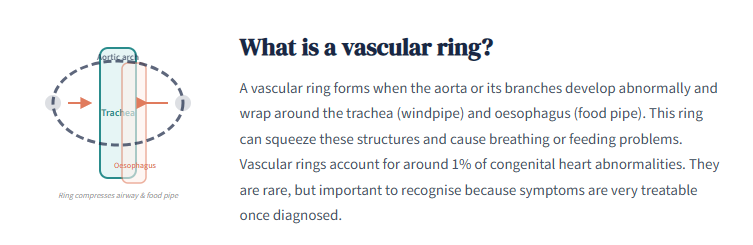
A vascular ring is a rare congenital abnormality in which the aorta or its branches develop in an unusual pattern and form a ring around the trachea (windpipe) and oesophagus (food pipe). This ring can squeeze one or both of these structures and cause problems with breathing, swallowing or feeding. Vascular rings account for around 1% of congenital cardiovascular abnormalities, and although they are uncommon, they are an important diagnosis to consider when a child has persistent respiratory or feeding symptoms that do not respond to standard treatment.
Some vascular rings form a complete circle around the airway and oesophagus, while others only partly surround them. Even an incomplete ring can cause significant symptoms if the compression is tight enough. The good news is that vascular rings are very treatable, and most children do extremely well once the diagnosis is made and, if needed, the compression is relieved.
The concern with a vascular ring is not usually the heart itself, which in most cases functions normally. The problem lies in the pressure that the abnormal vessels place on the airway and food pipe. This compression can lead to noisy breathing, stridor (a harsh, high-pitched sound during breathing), persistent cough, choking, swallowing difficulties and feeding problems. Some children develop symptoms that closely resemble asthma or gastro-oesophageal reflux but do not improve properly with the usual treatments.
This is one of the most important practical points for parents. Vascular rings are sometimes missed or diagnosed late because the symptoms overlap with much more common childhood conditions. Dr Giardini frequently sees children who have been treated for asthma or reflux for months before a vascular ring is identified as the true cause.
Symptoms vary depending on how tight the ring is and whether it is pressing more on the airway, the oesophagus or both.
Breathing symptoms often include noisy breathing or stridor, a persistent cough that does not settle, wheeze that does not follow the usual pattern of asthma, recurrent chest infections and breathing that sounds worse during feeding, crying or viral illnesses.
Feeding and swallowing symptoms may include choking or gagging during feeds, coughing while eating, slow or effortful feeding, reflux-like symptoms that do not respond well to treatment, difficulty swallowing and trouble with textured or solid foods. Swallowing difficulties sometimes become more obvious when a baby moves on from milk to solids, which can be the first clue that something other than reflux is at play.
In young babies, vascular rings may present with noisy breathing from the first weeks of life, feeding difficulty, distress during feeds and poor weight gain. In older children, symptoms may be more subtle, with swallowing problems or a persistent cough being the main concern.
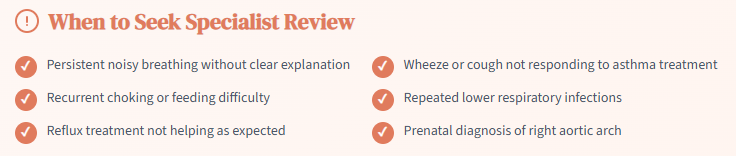
A vascular ring should be considered if a child has persistent noisy breathing that does not have a clear explanation, cough or wheeze that does not behave like typical asthma, feeding difficulty or choking that is not improving, repeated lower respiratory tract infections, reflux treatment that does not seem to be working, symptoms that become more noticeable when solids are introduced, or a prenatal diagnosis of a right aortic arch or possible vascular ring. If any of these features sound familiar, Dr Giardini can help determine whether further investigation is warranted.
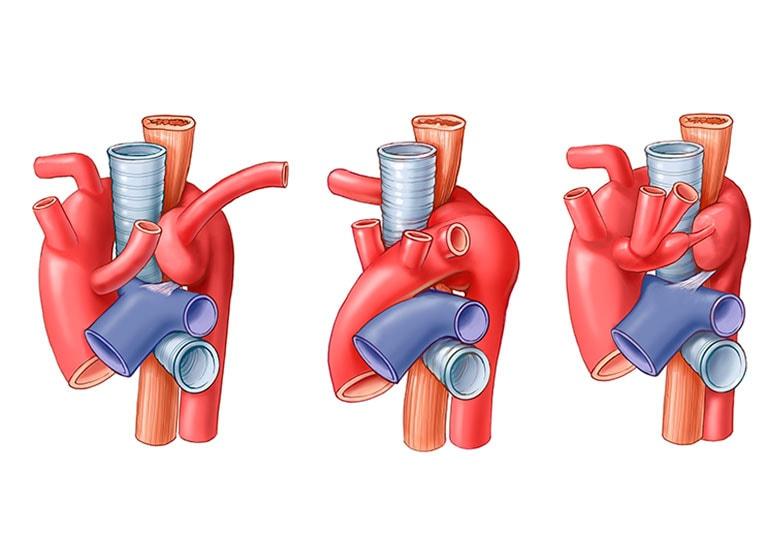
The two types that parents are most likely to hear about are the double aortic arch and the right aortic arch with aberrant left subclavian artery.
In a double aortic arch, the aorta divides into two branches that pass on either side of the trachea and oesophagus before joining together again, forming a complete ring. This is one of the classic and often more compressive forms of vascular ring, and children with this anatomy tend to present earlier in life.
In a right aortic arch with aberrant left subclavian artery, the aorta arches to the right instead of the left. An abnormal course of the left subclavian artery, combined with a ligament (the ligamentum arteriosum, a remnant of a fetal blood vessel), completes the ring around the airway and oesophagus. This variant is commonly identified on prenatal scans when a right-sided aortic arch is seen. Together, these two types account for the large majority of complete vascular rings. There are other rarer forms, but for most families these are the key patterns to understand.
Yes. A right aortic arch or a suspected vascular ring is sometimes identified on foetal ultrasound scans. This can understandably cause a great deal of anxiety for parents, but it is important to know that a prenatal finding does not automatically mean that the baby will be unwell or need urgent surgery after delivery. Many babies with a right aortic arch identified before birth do not develop significant symptoms straight away, and the key question after delivery is whether the anatomy is causing meaningful compression. Dr Giardini can assess your baby after birth with an echocardiogram and, if needed, arrange further imaging to clarify the anatomy and guide management.
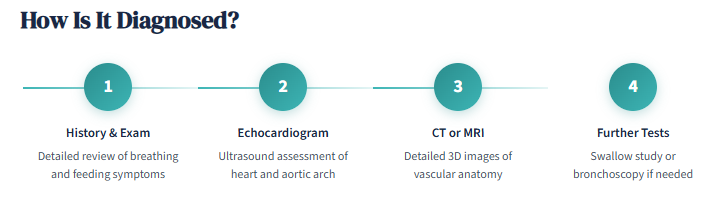
Diagnosis begins with a careful history and clinical examination. Dr Giardini will ask in detail about the pattern of breathing symptoms, feeding difficulties and any previous treatments that have been tried. The combination of airway and swallowing symptoms in the same child is often the clinical clue that raises suspicion.
Investigations may include an echocardiogram to assess the heart and aortic arch, a CT scan or MRI to provide detailed three-dimensional images of the vascular anatomy and its relationship to the airway and oesophagus, swallowing studies to look for oesophageal compression, and bronchoscopy in selected cases to directly visualise the airway. CT and MRI are particularly valuable because they show the exact anatomy of the ring and the degree of compression, which is essential information when planning treatment.
No. Some vascular rings are found incidentally, for example during investigation of an unrelated problem, and do not cause enough compression to require treatment. If your child has no symptoms and imaging shows only mild or no compression, Dr Giardini may recommend regular monitoring rather than surgery. Published outcome data support this approach, confirming that careful observation is safe for children who are genuinely asymptomatic.
Surgery is usually recommended when there are clear symptoms, such as noisy breathing, stridor, significant feeding problems, choking or evidence of meaningful airway or oesophageal compression on imaging.
The standard treatment is surgery to divide the ring and relieve the compression on the airway and oesophagus. The operation is not open-heart surgery. In most cases, the surgeon accesses the ring through an incision on the left side of the chest, passing between the ribs. The exact procedure depends on the type of vascular ring: in a double aortic arch, the smaller of the two arches is divided and stitched closed; in a right aortic arch with aberrant subclavian artery, the ligamentum arteriosum is divided and any compressive tissue is released.
The results of surgery are excellent. Large published series report that around 90% of children are free of ring-related symptoms at follow-up, and the procedure carries a very low complication rate. Most children spend only a few days in hospital after the operation.
It is worth knowing that recovery is not always instant, particularly if the airway has become floppy over time because of long-standing compression, a condition known as tracheomalacia. Some children continue to have noisy breathing or mild wheeze for weeks to months after surgery as the airway gradually regains its normal tone. This is well recognised and generally improves with time.
The outlook for children with vascular rings is very reassuring. The large majority do extremely well after surgical repair, with significant and lasting improvement in breathing, feeding and overall comfort. Some children need longer follow-up because of residual tracheomalacia, ongoing swallowing difficulties or more complex arch anatomy, but these issues are manageable and tend to improve over time.
Children who do not require surgery are monitored by Dr Giardini to ensure that symptoms do not develop as they grow. If the anatomy remains non-compressive, the long-term outlook is excellent without any intervention.
As a Consultant Paediatric Cardiologist at Great Ormond Street Hospital and in private practice in London, Dr Giardini regularly assesses children with congenital aortic arch abnormalities, noisy breathing, feeding difficulties and suspected vascular rings. The key is to determine whether the anatomy is truly forming a ring, whether it is causing meaningful compression, and whether symptoms are mild, evolving or significant enough to need treatment.
If your child has been diagnosed with a vascular ring, or if you are looking for a second opinion because symptoms do not quite fit asthma or reflux, you are very welcome to contact Dr Giardini's team to arrange a specialist review.
A vascular ring is an abnormal arrangement of the aorta or its branches that wraps around and can compress the windpipe, the food pipe or both. It is a congenital condition, meaning it develops before birth.
Yes. Noisy breathing and stridor are among the most common symptoms, particularly in younger children. The noise is caused by the ring pressing on the outside of the airway.
Yes. The symptoms of airway compression can closely resemble asthma or reactive airway disease. If inhaler treatment is not working as expected, a vascular ring should be considered.
Yes. Many children have choking, coughing with feeds, reflux-like symptoms or difficulty swallowing, particularly with solid foods. These symptoms occur because the ring also compresses the oesophagus.
No. Some children with a vascular ring have no symptoms and require only regular monitoring. Surgery is recommended when the ring is causing clear symptoms or significant compression.
CT or MRI provides the most detailed images of the vascular anatomy and the degree of airway and oesophageal compression. An echocardiogram is also used to assess the heart and aortic arch.
Yes. A right aortic arch or suspected vascular ring may be identified on foetal ultrasound. This does not necessarily mean the baby will need surgery, and postnatal assessment will clarify the anatomy.
The two most common complete vascular rings are the double aortic arch and the right aortic arch with aberrant left subclavian artery and ligamentum arteriosum.
Most children improve very significantly. Some continue to have mild airway symptoms for a while, particularly if tracheomalacia (floppiness of the airway) has developed from long-standing compression. This usually improves with time.
If your child has persistent noisy breathing, feeding difficulty, choking, recurrent chest infections, or a suspected vascular ring on prenatal or postnatal imaging, specialist review with Dr Giardini is recommended.
Author: Dr. Alessandro Giardini, MD, PhD, Consultant Paediatric Cardiologist
Written 22/04/2026
Last reviewed 03/07/2026