
Dr. Alessandro Giardini
If your child has been diagnosed with rheumatic fever or rheumatic heart disease, it is natural to feel concerned, particularly when you hear that a throat infection can affect the heart.
The most important thing to understand is this: rheumatic heart disease is largely preventable, and when recognised early, doctors can manage it effectively and reduce the risk of long-term complications.
I'm Dr Alessandro Giardini, Consultant Paediatric Cardiologist at Great Ormond Street Hospital and the Portland Hospital. I assess children with suspected or confirmed heart involvement following infections and help families understand what needs treatment, what can safely be monitored, and how to protect the heart going forward.
This is an important question, and the answer depends largely on when doctors recognise the condition and how effectively they manage it over time.
During rheumatic fever, inflammation affecting the heart valves can be mild and may settle completely with treatment. Many children do not go on to develop lasting heart problems. More significant disease tends to arise when rheumatic fever goes undetected, untreated, or recurs, leading to gradual scarring of the valves.
The key point is that rheumatic heart disease is both preventable and manageable. Prompt treatment of throat infections and appropriate long-term follow-up where needed greatly reduce the risk of serious complications, and many children go on to live normal, active lives.
This is often the key question behind the diagnosis, and it surprises most parents.
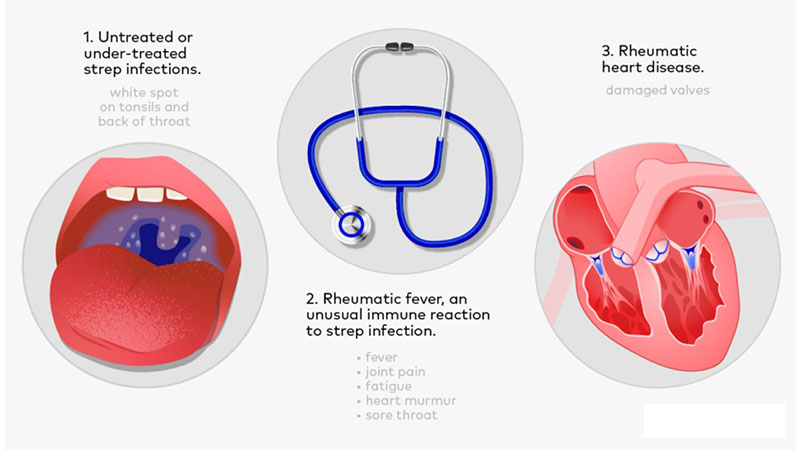
Rheumatic heart disease develops as a delayed complication of a throat infection caused by a specific type of bacteria called group A streptococcus (the same bacteria that cause "strep throat" and scarlet fever). In a small number of children, the immune system fights the infection but then mistakenly turns against the body's own tissues, including the heart valves. This immune overreaction is called rheumatic fever.
Not every sore throat carries this risk. Only untreated or undertreated streptococcal throat infections can trigger rheumatic fever, and even then, fewer than 1 in 300 children with strep throat develop it. Most sore throats in children are viral and carry no risk at all.
The key fact for parents is straightforward: prompt antibiotic treatment of strep throat almost entirely eliminates the risk of rheumatic fever. This makes rheumatic heart disease one of the few heart conditions that is genuinely preventable.
When rheumatic fever affects the heart, the immune system's antibodies attack the heart valve tissue because its protein structure closely resembles the streptococcal bacteria (a process doctors call molecular mimicry). This causes inflammation of the valve leaflets, a condition called carditis.
The mitral valve, which sits between the two left chambers of the heart, bears the brunt of this attack in most children. The aortic valve can also become involved, though less commonly. During the acute phase, inflammation can make the valve leaflets swollen and leaky. If the inflammation settles quickly with treatment, the valves may recover fully.
Repeated episodes of rheumatic fever pose the greatest danger. Each new attack adds fresh inflammation on top of previous scarring. Over months and years, this can gradually thicken and stiffen the valve leaflets, eventually narrowing the valve opening (stenosis) or preventing it from closing properly (regurgitation). This progressive valve damage is what doctors call rheumatic heart disease.
The interval between the initial infection and the appearance of significant valve disease can stretch over many years. Some people develop symptoms of valve damage only 10 to 20 years after their original episode of rheumatic fever.
In the UK and other high-income countries, rheumatic fever has become uncommon thanks to widespread access to antibiotics and clean living conditions. Before penicillin became widely available, rheumatic heart disease was a leading cause of childhood heart problems and early death.
Globally, the picture looks very different. Rheumatic heart disease remains the most common acquired heart condition in children and young adults worldwide, affecting an estimated 40 million people and causing around 300,000 deaths each year. The burden falls heaviest on children in sub-Saharan Africa, South Asia, the Pacific Islands and among Indigenous populations in Australia and New Zealand.
For families in the UK with roots in or regular travel to higher-prevalence regions, awareness matters. I see children in my practice whose families have connections to these areas, and understanding the risk helps ensure that strep throat receives prompt treatment wherever the child happens to be.
Children between 5 and 15 years of age face the highest risk of rheumatic fever. Younger children and adults rarely develop it. Several factors increase susceptibility: repeated strep throat infections, overcrowded living conditions, limited access to healthcare, and a family history of rheumatic fever or rheumatic heart disease. Girls and women face roughly twice the risk of developing rheumatic heart disease compared to boys and men, though the reasons for this remain unclear.
Symptoms depend on whether a child has acute rheumatic fever or more established valve involvement.
Symptoms typically appear about two to four weeks after a strep throat infection. Fever and general malaise are common. Joint pain and swelling often develop, characteristically moving from one large joint to another (migratory arthritis), affecting the knees, ankles, elbows or shoulders. A distinctive painless skin rash (erythema marginatum) may appear on the trunk, though this occurs in only a small proportion of children. Firm, painless nodules under the skin can occasionally develop near joints.
In a smaller number of children, the inflammation affects the brain, producing involuntary jerky movements known as Sydenham's chorea (sometimes called St Vitus' dance). These movements may appear weeks or even months after the original infection, sometimes after other symptoms have already resolved, and can affect concentration and handwriting.
When carditis develops during rheumatic fever, the doctor may detect a new heart murmur. Breathlessness and reduced exercise tolerance can occur if the valve leak is significant. Chest discomfort and a fast heartbeat are less common but possible. Some children have very mild carditis that produces no noticeable symptoms at all and only shows on echocardiography.
Children with progressive valve damage may develop ongoing fatigue, breathlessness on exertion, palpitations, or swelling of the ankles and abdomen due to fluid retention. These symptoms tend to emerge gradually as the valve damage advances, sometimes years after the acute illness.
GREEN: Usually reassuring. Your child had a simple sore throat with quick recovery, no persistent fever or joint symptoms, and remains active and well. No specific cardiac concern.
AMBER: Needs medical review. Your child has a persistent fever following a throat infection, joint pain or swelling, new tiredness or reduced activity, or a heart murmur identified on examination. Arrange medical assessment.
RED: Needs urgent assessment. Your child has breathlessness at rest or with minimal activity, chest discomfort or palpitations, fainting episodes, or significant deterioration. Seek urgent medical attention.
%20(2).png)
Doctors diagnose rheumatic fever using a framework called the modified Jones criteria, which bring together clinical findings, blood tests and heart imaging. No single test can confirm the diagnosis on its own.
The criteria require evidence of a recent streptococcal infection (through a positive throat culture, rapid antigen test, or elevated blood antibodies such as ASO titre or anti-DNase B) together with a combination of characteristic features. Major criteria include carditis, migratory joint inflammation, chorea, the typical skin rash, and subcutaneous nodules. Minor criteria include fever, joint pain without frank swelling, raised inflammatory markers (ESR or CRP), and a prolonged PR interval on ECG.
An echocardiogram (heart ultrasound) is the most important cardiac investigation. It allows me to check whether the heart valves are inflamed or leaking, measure the degree of regurgitation, and look for any fluid around the heart (pericardial effusion). Echocardiography can detect valve involvement even when no murmur is audible, which is why I recommend it for every child with suspected rheumatic fever. An ECG helps identify any electrical conduction changes.
Treatment targets three goals: eliminating the infection, controlling inflammation, and preventing recurrence.
Antibiotics, most commonly penicillin, clear the streptococcal bacteria. Completing the full course matters even if your child feels better within a day or two.
Anti-inflammatory treatment reduces the immune reaction affecting the joints and heart. High-dose aspirin is the standard first-line treatment for joint inflammation. When significant carditis is present, corticosteroids may be needed to bring the cardiac inflammation under control more quickly.
This is arguably the most critical step in the entire management of rheumatic heart disease. Each recurrence of rheumatic fever can add further damage to already vulnerable heart valves. Long-term antibiotic prophylaxis, usually with regular penicillin injections every three to four weeks (or daily oral penicillin), dramatically reduces the risk of further streptococcal infections and therefore further attacks.
The duration of prophylaxis depends on whether heart involvement occurred. Children with valve damage typically continue prophylaxis for at least 10 years after the last episode, and often well into adulthood. Children who had rheumatic fever without heart involvement may stop earlier, though guidelines vary and I discuss the individual plan carefully with each family.
When valve damage develops and progresses despite prevention, further treatment may include medication to support heart function (such as diuretics for fluid retention, or ACE inhibitors to reduce the workload on the heart), regular cardiac monitoring to track valve function over time, and, in more advanced cases, surgery to repair or replace the damaged valve. Valve surgery is uncommon in childhood but may become necessary later in life if the valve narrows significantly or the leak becomes severe enough to strain the heart.
Children with damaged heart valves face a higher risk of infective endocarditis, a serious infection of the heart valve. Good oral hygiene and regular dental check-ups play an important protective role. Some children may need antibiotic cover before certain dental procedures. I always discuss this with families as part of the overall care plan.
For most children, management involves regular follow-up rather than immediate intervention. This typically includes periodic echocardiograms to track valve function, clinical review of symptoms and exercise tolerance, and ongoing preventive antibiotic treatment. In many cases the condition remains stable or improves over time. Where changes occur, they tend to develop gradually and can be managed proactively.
I work with each family to build a clear, structured follow-up plan so that everyone understands what needs monitoring, what symptoms to watch for, and how to reduce future risk.
Yes, and this is one of the most important messages for families. Prompt treatment of strep throat with antibiotics almost entirely prevents rheumatic fever from developing. For children who have already had rheumatic fever, long-term antibiotic prophylaxis is highly effective at preventing recurrence and further valve damage.
Parents can help by recognising the signs of strep throat (sudden onset sore throat with fever, headache and sometimes abdominal pain, but typically no cough or runny nose), seeking medical assessment promptly, and ensuring that prescribed antibiotics are completed in full.
Most sore throats in children are viral, settle within a few days, and carry no risk to the heart. The situation to be more mindful of is a possible streptococcal (strep) throat infection, as this is the type that can, rarely, lead to rheumatic fever if left untreated.
Seek medical advice if your child has a sudden onset of sore throat with fever, pain on swallowing, swollen neck glands, or a rash, particularly without the cough or runny nose that typically accompany viral infections. If strep throat is suspected, prompt antibiotics are highly effective at preventing rheumatic fever.
If your child has previously had rheumatic fever, seek advice early for any sore throat, ensure all prescribed antibiotics are completed in full, and continue any long-term preventive antibiotics as advised.
The key is simply recognising when a throat infection might need medical attention, so that treatment can start early and the risk to the heart remains extremely low.
This is a very natural concern, particularly when you hear that rheumatic fever can affect the heart valves.
The answer depends mainly on whether the heart was involved during the initial illness, and how effectively future episodes are prevented.
Many children who have rheumatic fever do not develop lasting heart damage at all. When doctors recognise mild valve inflammation early, treatment can lead to a complete recovery. More significant valve involvement may leave some degree of long-term change, such as mild leakage or gradual thickening of the valve leaflets. In many cases, these changes remain stable and manageable with regular follow-up.
Recurrent episodes of rheumatic fever pose the greatest risk, as each attack can add further damage. Long-term antibiotic prevention plays a critical role in protecting the heart going forward.
Even children who develop valve changes can usually be followed safely for many years. Any intervention, if ever needed, is typically planned carefully rather than performed urgently. A clear follow-up plan allows us to detect changes early and act before they become a problem.
In most cases, yes. Children who receive early diagnosis and appropriate management attend school normally, take part in everyday activities, and have a good long-term outlook. Some may need ongoing monitoring into adulthood, particularly if valve changes develop, but many live full and active lives. I always aim to give families a realistic picture of what to expect while focusing on the positive steps that can make the biggest difference.
You should consider specialist review if your child has been diagnosed with rheumatic fever, there is concern about heart involvement, a murmur has been detected after an illness, symptoms such as breathlessness or fatigue persist following a throat infection, or your child has a history of rheumatic fever and you want an updated assessment of the heart valves.
I provide detailed cardiac assessment with echocardiography, clear explanation of findings and what they mean for your child, structured follow-up plans including coordination of preventive treatment, and guidance on oral hygiene, exercise and long-term outlook. Most importantly, I help families understand what matters, what does not, and how to move forward with confidence.
Very rarely. Only specific untreated streptococcal throat infections can trigger rheumatic fever. Most sore throats in children are viral and carry no risk to the heart. When strep throat is treated promptly with antibiotics, the risk of rheumatic fever drops to near zero.
Rheumatic fever and rheumatic heart disease have become uncommon in the UK thanks to widespread antibiotic use. Globally, however, the condition remains the most common acquired heart disease in children and young adults, affecting around 40 million people. Families with connections to higher-prevalence regions should stay aware of the risk.
Rheumatic fever is an inflammatory reaction triggered by the immune system after a strep throat infection. The immune system's antibodies attack the body's own tissues, including the heart valves, because their protein structure resembles the bacteria. Repeated episodes can scar and damage the valves permanently.
Doctors use the modified Jones criteria, combining evidence of recent strep infection with characteristic clinical features such as joint inflammation, carditis, chorea, or skin changes. Blood tests check for strep antibodies and inflammatory markers. An echocardiogram assesses whether the heart valves have been affected.
Long-term antibiotic prophylaxis prevents new strep infections from triggering further episodes of rheumatic fever. Each recurrence can worsen valve damage, so prevention is critical. Children with valve involvement typically continue prophylaxis for at least 10 years and often into adulthood.
Most children do not. Surgery is only considered when valve damage progresses to the point where it significantly affects heart function, and this is uncommon in childhood. When needed, surgeons can often repair the valve rather than replace it.
Rheumatic fever itself can recur if a child has another untreated strep infection, and each recurrence risks adding more damage. This is exactly why preventive antibiotics are so important. With consistent prophylaxis, the risk of recurrence drops dramatically.
In most cases, yes. Children with mild or no valve involvement can take part in normal physical activities. Those with more significant valve disease may need some guidance on exercise intensity. I assess each child individually and give tailored advice.
Sydenham's chorea involves involuntary jerky movements that can appear weeks or months after rheumatic fever. It may affect coordination, handwriting and concentration. Although alarming to witness, it typically resolves over weeks to months and does not cause lasting neurological damage. It does confirm that the immune system reacted to strep, and the child should receive standard cardiac assessment.
Children with damaged heart valves face a higher risk of infective endocarditis, a serious infection that can develop when bacteria from the mouth enter the bloodstream. Good daily oral hygiene and regular dental check-ups provide important protection. Some children may also need antibiotic cover before certain dental procedures.
Author: Dr. Alessandro Giardini, MD, PhD
Written 04/05/2026