
Dr. Alessandro Giardini
If your baby or child has been diagnosed with Ebstein anomaly, you will almost certainly have questions about what it means and what happens next. The condition varies enormously from one child to another, and that can make it feel difficult to know what to expect.
The most important thing to understand is this: with expert assessment and the right care plan, the large majority of children with Ebstein anomaly grow up to live active, fulfilling lives.
I'm Dr Alessandro Giardini, Consultant Paediatric Cardiologist at Great Ormond Street Hospital. I regularly look after children with Ebstein anomaly and help families navigate everything from initial diagnosis through to long-term follow-up, including decisions about surgery and exercise.
Ebstein anomaly is a rare congenital heart defect affecting the tricuspid valve, which sits between the two chambers on the right side of the heart. It occurs in approximately 1 in 20,000 babies.
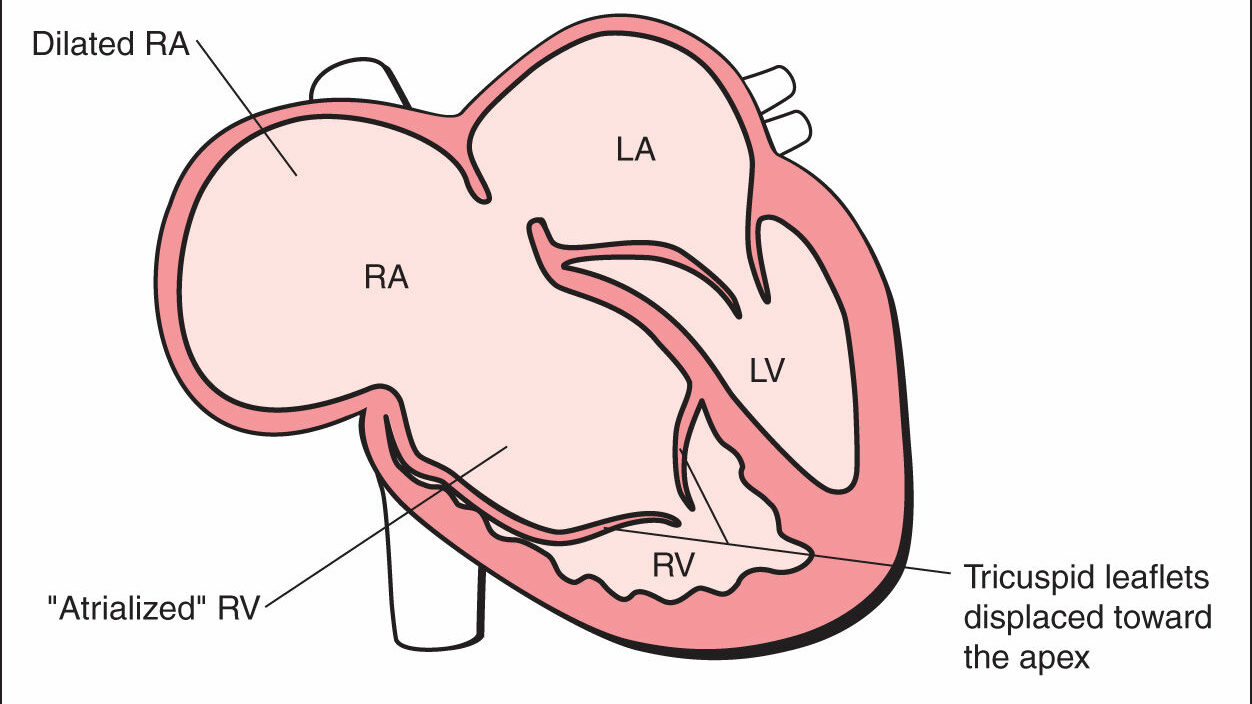
In a normal heart, the tricuspid valve opens to let blood flow from the right atrium (collecting chamber) into the right ventricle (pumping chamber), then closes tightly to prevent blood leaking backwards. In Ebstein anomaly, the valve leaflets sit lower than they should, displaced downward into the right ventricle. This creates three problems: the valve leaks (tricuspid regurgitation), the right atrium becomes enlarged, and part of the right ventricle effectively becomes thin-walled and unable to pump properly.
The severity ranges widely. Some children have a very mild form with minimal or no symptoms and may never need treatment. Others have a more significant defect that requires medication, close monitoring, or surgery. This wide range means that every child's care plan looks different, and understanding your child's specific anatomy is the essential first step.
Many children with Ebstein anomaly also have other heart findings. An atrial septal defect (a hole between the upper chambers) or a patent foramen ovale is common. Some children have pulmonary valve problems, and around 10 to 25 per cent have an extra electrical pathway in the heart called Wolff-Parkinson-White (WPW) syndrome, which can cause episodes of very fast heart rate.
Ebstein anomaly develops during the first weeks of pregnancy, typically between weeks 6 and 10, when the tricuspid valve is forming. The valve leaflets fail to separate properly from the heart muscle wall and do not move into their correct position.
In the vast majority of cases, no specific cause can be identified. Nothing you did or did not do during pregnancy caused your child's condition, and parents should not feel responsible for the diagnosis. This is an important point that I always discuss with families.
Researchers have identified a small number of factors that may increase risk. Lithium use during early pregnancy is the most established association. Poorly controlled maternal diabetes and exposure to certain other medications may also play a role. Most cases, however, occur without any identifiable risk factor at all.
Ebstein anomaly is usually sporadic, meaning it happens by chance rather than running in families. Familial cases do occur rarely, and genetic counselling may help if you have a family history of congenital heart disease or are planning future pregnancies.
Symptoms depend entirely on severity. Some children have no symptoms at all, while others need urgent care from birth.
In newborns and babies, the most common sign is a blue tinge to the skin, lips or nail beds (cyanosis), caused by lower oxygen levels in the blood. Rapid breathing, difficulty feeding, poor weight gain and a heart murmur picked up on examination can all point to the diagnosis. Babies with the most severe forms may need intensive care support from birth.
In older children and teenagers, symptoms tend to be more subtle. Fatigue and reduced stamina during physical activity are common. Palpitations or awareness of a fast or irregular heartbeat may occur, particularly in children who have WPW syndrome. Breathlessness on exertion, chest discomfort and dizziness or fainting are less common but should always prompt assessment.
Some children remain well for years and receive their diagnosis only when a doctor hears a murmur during a routine check or investigates another problem. A mild form may cause no limitation at all in childhood.
GREEN: Usually reassuring. Your child has mild Ebstein anomaly, no symptoms, normal oxygen levels and stable heart size on scans. Regular follow-up with your paediatric cardiologist is all that's needed.
AMBER: Needs specialist review. Your child shows new or worsening symptoms such as reduced exercise tolerance, palpitations or breathlessness. The heart appears to be enlarging on echocardiography, or your child has episodes of fast heart rate. Arrange a cardiology review.
RED: Needs urgent assessment. Your baby has a blue colour change, difficulty breathing or feeding problems. An older child collapses, faints, or experiences a prolonged episode of very fast heart rate. Seek urgent medical attention.
.png)
Doctors can sometimes detect Ebstein anomaly before birth during a routine pregnancy ultrasound, usually after 18 to 20 weeks. A foetal echocardiogram then provides more detail about the heart.
After birth, the primary diagnostic tool is an echocardiogram (heart ultrasound). This painless test shows exactly where the valve sits, how badly it leaks, how large the right atrium has become, and whether the right ventricle is pumping effectively. It also identifies any associated defects such as holes in the heart or pulmonary valve problems.
An ECG (electrocardiogram) checks the heart's electrical activity. Most children with Ebstein anomaly show characteristic changes on ECG, and the test can reveal whether WPW syndrome or other rhythm abnormalities are present.
Cardiac MRI provides detailed information about the size and function of both ventricles and plays a particularly important role when surgery is being considered. I use MRI routinely for pre-operative planning and for long-term monitoring in older children.
Doctors classify severity using several systems. The Carpentier classification describes the anatomy of the valve, ranging from mild displacement with good leaflet movement (Type A) through to near-complete absence of functional valve tissue (Type D). Functional scoring systems such as the Great Ormond Street Score combine anatomical and functional measures to guide treatment decisions.
Treatment is highly individual. Some children never need anything beyond regular monitoring, while others require medication, catheter procedures, or surgery. The approach depends on the severity of the valve problem, the child's symptoms, how well the right ventricle works, and whether rhythm disturbances are present.
Many children with mild or moderate Ebstein anomaly do well with careful surveillance alone. This involves regular cardiology appointments, serial echocardiography to track valve function and heart size, ECG monitoring for rhythm problems, and exercise testing to assess how the heart copes with activity. Most children in this group attend school normally and take part in everyday activities without difficulty.
When symptoms develop, several medications can help. Diuretics reduce fluid build-up if the heart is working under strain. ACE inhibitors or ARBs help reduce the workload on the right ventricle. Anti-arrhythmic medications such as flecainide or sotalol can control abnormal heart rhythms. Beta-blockers may also help with rhythm management in some children.
For children with WPW syndrome, radiofrequency ablation can eliminate the extra electrical pathway causing fast heart rates. This catheter-based procedure often provides a permanent cure for the rhythm problem. Where an atrial septal defect needs closing and the anatomy is suitable, doctors can sometimes close it using a catheter-delivered device rather than open surgery.
When the valve leak becomes significant, the right ventricle is struggling, or symptoms are progressing despite medication, surgery offers the best path forward. The key question is whether the valve can be repaired or whether it needs replacing.
Cone repair has transformed the surgical treatment of Ebstein anomaly and represents the current gold standard. Pioneered by Dr José Pedro da Silva and further developed at centres including Great Ormond Street Hospital, this technique mobilises all available valve leaflet tissue and reconstructs it into a cone-shaped apparatus sitting at the correct position. The result is a functioning valve built from the child's own tissue.
Results from cone repair are excellent. Studies show hospital mortality rates of around 3 per cent for elective procedures, with significant improvement in valve function after surgery. Right ventricular size typically decreases over the following months as the heart remodels, and most children experience a genuine improvement in exercise capacity and quality of life. Long-term data shows 85 to 95 per cent freedom from reoperation at 10 years.
Not every child is suitable for cone repair. When the valve tissue is too severely abnormal or insufficient for reconstruction, valve replacement becomes necessary. Surgeons generally prefer bioprosthetic (tissue) valves in younger patients, as these avoid the need for lifelong blood-thinning medication.
In the most severe cases, particularly in newborns whose right ventricle cannot support a full circulation, surgeons may need to consider staged procedures or, very rarely, heart transplantation.
Babies born with severe Ebstein anomaly may need prostaglandin infusions to keep a crucial blood vessel (the ductus arteriosus) open, along with ventilator support and intensive monitoring. The approach of stenting the PDA in this setting has also been employed succesfully in very selected cases. Decisions about the timing and type of intervention in these tiny patients require careful multidisciplinary discussion, and I work closely with our cardiac surgical and intensive care teams to plan the safest approach.
Rhythm problems deserve particular attention throughout life. Around a quarter of people with Ebstein anomaly develop arrhythmias at some point. Regular Holter monitoring (24-hour ECG recording) helps detect problems early, and electrophysiology studies may be needed before or during surgical repair.
Ebstein anomaly covers a wide spectrum. Some children have a very mild form with little valve leakage, normal oxygen levels and no impact on daily life. These children often grow up without significant limitations. At the other end, particularly in newborns with more severe forms, the condition can affect how well the heart delivers blood to the lungs, causing a blue colour, breathing difficulties or feeding problems that may require early treatment.
Most children fall somewhere in between. They may have a degree of valve leakage or an enlarged right heart but remain well for long periods with careful follow-up. Some will eventually need medication or surgery, often later in childhood rather than in infancy.
Ebstein anomaly is not one condition with a single outcome. What matters is your child's specific anatomy, how the heart copes, and how things change over time. A specialist assessment clarifies where your child sits on this spectrum and what needs action now versus what simply needs watching.
This is one of the first questions parents ask, and understandably so. The answer depends on how severe the Ebstein anomaly is in your baby.
Many babies with milder forms do not need surgery at all. Careful monitoring with regular scans is often enough, and these children frequently grow and develop well without intervention. For babies with more significant valve leakage or symptoms such as breathlessness, poor feeding or low oxygen levels, treatment may come earlier. Sometimes medication alone supports the heart effectively. In a smaller group, surgery offers the best path to improving valve function and overall heart performance.
When surgery is needed, the team usually plans it carefully rather than performing it as an emergency. Modern techniques, particularly cone repair, have significantly improved outcomes. The goal is always to intervene at the right time, before the heart begins to struggle but not before it is truly necessary.
One of the most important parts of specialist care is helping you understand where your child sits on this spectrum and what to expect as they grow.
For most children, yes. Children with mild Ebstein anomaly often live completely unrestricted lives. Those who undergo successful surgical repair typically experience significant symptom relief and can return to normal activities. Most children attend school as usual, and many take part in recreational sport with appropriate guidance.
Exercise recommendations depend on the severity of the condition and the state of the valve. I assess each child individually and provide clear advice on what activities are safe, always aiming to keep children as active as possible while staying within safe limits.
All children with Ebstein anomaly need lifelong cardiology follow-up, regardless of severity. Hearts can change over time, and new rhythm problems can develop even in adulthood. The transition from paediatric to adult congenital heart disease services is an important step that I help families plan for well in advance.
You should seek review if your baby has a heart murmur or blue colour changes, your child has unexplained exercise limitation or palpitations, you have received a prenatal diagnosis of Ebstein anomaly and want expert counselling, your child needs assessment before any planned surgery, or you simply want a specialist opinion and clear guidance.
Ebstein anomaly is a rare congenital heart defect where the tricuspid valve sits lower than normal inside the right ventricle. This causes the valve to leak and the right side of the heart to work less efficiently. It affects approximately 1 in 20,000 babies and varies enormously in severity.
No. In the large majority of cases, no specific cause can be identified. The condition develops during the early weeks of pregnancy due to a random variation in how the tricuspid valve forms. Nothing you did or did not do caused it, and you should not feel responsible.
Not necessarily. Many children with mild Ebstein anomaly never need surgery and do well with monitoring alone. When surgery is needed, the cone repair technique offers excellent results, with most children experiencing significant improvement in valve function, exercise capacity and quality of life.
Cone repair is the current gold standard operation for Ebstein anomaly. The surgeon mobilises all available valve leaflet tissue and reconstructs it into a cone shape at the correct position. This creates a functioning valve from the child's own tissue, avoiding the need for an artificial valve in most cases. Studies report very good outcomes with low reoperation rates over the following decade.
Older data quoting an average life expectancy of 25 to 30 years reflected a time before modern surgical techniques existed, and included the most severe cases. With current treatment, particularly cone repair surgery, the outlook has improved dramatically. Many people with Ebstein anomaly now live well into adulthood, and children with milder forms can expect a near-normal lifespan.
Many children with Ebstein anomaly can take part in physical activities and recreational sport. The level of activity depends on the severity of the valve problem and how well the right ventricle functions. I assess each child individually and provide tailored guidance, always aiming to keep children as active as safely possible.
About 10 to 25 per cent of children with Ebstein anomaly have an extra electrical pathway in the heart called WPW syndrome. This can cause episodes of very fast heart rate (supraventricular tachycardia). An ECG can detect the characteristic pattern, and radiofrequency ablation often provides a permanent cure for the rhythm problem.
The frequency depends on severity. Children with mild forms may need annual or biannual appointments. Those with more significant valve problems, enlarging hearts or rhythm issues may need more frequent visits. Regular echocardiography and ECG monitoring form the core of ongoing surveillance.
Most cases occur by chance and do not run in families, so routine screening of siblings is not usually necessary. If there is a broader family history of congenital heart disease or a known genetic condition, your cardiologist or geneticist can advise on whether assessment of other family members would be helpful.
Some children with Ebstein anomaly need antibiotic prophylaxis before certain dental or surgical procedures to reduce the risk of infective endocarditis (an infection of the heart). Good oral hygiene also plays an important role in prevention. Your cardiologist can advise whether this applies to your child.
Author: Dr. Alessandro Giardini, MD, PhD
Written 30/03/2026