
Dr. Alessandro Giardini
A sharp chest pain that worsens lying down and eases sitting forward is a pattern worth taking seriously. It is the hallmark presentation of pericarditis, and recognising it early matters because the condition is treatable and the outcome is excellent when managed properly.
Most children with pericarditis recover fully with rest and a short course of anti-inflammatory medication. A smaller group develops complications or recurrent episodes requiring specialist input. Understanding which group your child falls into is the primary goal of assessment.
The pericardium is a two-layered sac that surrounds and protects the heart. Between its inner and outer layers lies a thin film of fluid that allows the heart to beat freely without friction. Pericarditis occurs when these layers become inflamed. The inflammation produces chest pain, sometimes a small collection of fluid around the heart, and characteristic changes on the ECG.
The condition is distinct from myocarditis, which involves inflammation of the heart muscle itself rather than the surrounding sac. Both can occur at the same time, a combination sometimes called myopericarditis.
Viral infection is the most common cause in children and teenagers, accounting for the majority of cases. Coxsackieviruses, enteroviruses, influenza, Epstein-Barr virus, and adenovirus are among the most frequently implicated. In many children, pericarditis develops one to two weeks after an apparently ordinary respiratory or gastrointestinal illness. The virus itself is often never specifically identified.
Children who have undergone open-heart surgery for congenital heart defects carry a particular risk of pericarditis in the weeks to months after the operation. This is known as post-pericardiotomy syndrome, and it develops because surgery triggers an immune response against the pericardium. It can occur after procedures to repair ventricular or atrial septal defects, Tetralogy of Fallot, and other structural conditions. Parents whose children have undergone cardiac surgery should be aware of this possibility.
Pericarditis can be a manifestation of systemic autoimmune diseases including juvenile idiopathic arthritis, systemic lupus erythematosus, and familial Mediterranean fever. In these cases the pericarditis tends to be part of a broader pattern of inflammation affecting multiple organs. Identifying the underlying condition changes the management approach as specific treatment for the condition resolves the pericardial inflammation.
Bacterial pericarditis is rare but serious. When it occurs, it tends to produce a large pericardial effusion rapidly and the child is typically more unwell than with viral pericarditis. Staphylococcus aureus and Streptococcus pneumoniae are among the organisms involved. This form requires hospitalisation and intravenous antibiotics. Prolonged bacterial infections can also cause the pericardium to stiffen permanently, causing a condition called constructive pericarditis.
COVID-19 infection can trigger pericarditis directly. Multisystem inflammatory syndrome in children (MIS-C), a serious post-COVID inflammatory condition, may also involve the pericardium alongside the heart muscle. Reports have additionally documented pericarditis as a rare adverse event following mRNA COVID-19 vaccination, particularly in adolescent males. This is uncommon and typically mild. Cardiac symptoms following recent COVID illness or vaccination warrant assessment.
The positional chest pain of pericarditis has a quality that distinguishes it from most other childhood chest pain. It is typically sharp, often felt behind the breastbone or in the left chest, and it worsens noticeably when the child lies flat on their back. Sitting upright and leaning slightly forward relieves it. This pattern alone is diagnostically helpful.
Younger children often cannot describe the pain precisely. Irritability, reluctance to lie flat, refusing to feed normally, and unusual fatigue are the signs parents notice first. The connection to a chest problem may not be immediately apparent.
Breathing adds another dimension. Deep breaths often make the pain worse, which is why children with pericarditis sometimes breathe shallowly and prefer to remain still. A cough that develops alongside the inflammation produces sharp pain with each episode.
Fever is common. Many children have recently recovered from or are still experiencing an intercurrent illness. A pericardial friction rub, a scratching or leathery sound heard with the stethoscope when the inflamed layers move against each other, is a specific clinical finding when present. It is not always audible.
A child with chest pain that is positional, worsened by lying down, and has followed a recent viral illness should be assessed by a doctor on the same day.
Seek immediate assessment if chest pain is severe, if the child is breathless at rest, if breathing is noticeably laboured, if the heart is beating very fast, or if the child looks pale, grey, or feels faint. Children with any of these features need immediate assessment. They may indicate significant fluid around the heart.
Children who have previously had pericarditis and develop familiar symptoms again should be assessed promptly. Waiting is not the right response.
Dr Giardini provides same-day assessment including ECG and echocardiography at his London clinics, allowing a clear diagnosis and management plan to be established during a single appointment.
No single test diagnoses pericarditis on its own. Diagnosis rests on combining the clinical history, examination findings, and investigation results.
The electrocardiogram is one of the most useful initial investigations. In acute pericarditis, the ECG shows a characteristic pattern of widespread ST elevation with a concave or saddle-shaped appearance, often accompanied by PR segment depression. These changes differ from the ST elevation seen in a heart attack and from the changes seen in myocarditis alone.
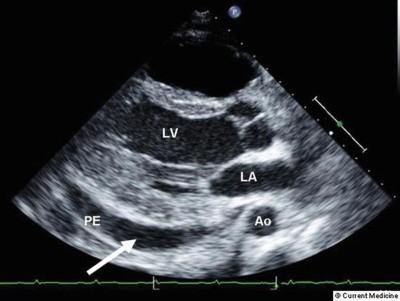
The echocardiogram detects pericardial effusion, assesses its size, and evaluates how well the heart is functioning within the fluid. It is essential when any significant fluid collection is suspected and provides immediate guidance on whether drainage is needed.
C-reactive protein (CRP) is the most useful marker of pericardial inflammation. An elevated CRP at presentation also predicts a higher risk of recurrence. Troponin levels help determine whether the heart muscle itself has been affected alongside the pericardium, as occurs in myopericarditis. Full blood count, renal function, autoimmune screens, and viral serology are included in the workup where indicated.
Cardiac MRI provides detailed images of pericardial inflammation and is particularly useful when the diagnosis is uncertain or when myopericarditis is suspected. It can also detect pericardial thickening in children being assessed for constrictive pericarditis.
Ibuprofen is the first-line treatment for most children with viral or idiopathic pericarditis. Taken at the appropriate dose and on a regular schedule for the prescribed duration, it substantially reduces pain and inflammation. Aspirin is an alternative, particularly in children who have recently had cardiac surgery.
Continue treatment until symptoms have settled and CRP has returned to normal. Tapering the dose too quickly is one of the commonest reasons for early relapse.
Colchicine, an anti-inflammatory medication derived from the autumn crocus, significantly reduces the risk of pericarditis recurring. Evidence from adult trials demonstrates a roughly 50 per cent reduction in recurrence rates when clinicians add colchicine to anti-inflammatory treatment from the outset. Growing paediatric evidence now supports its use in children. Doses are adjusted for age and weight. Gastrointestinal side effects are the most common concern.
Children with active pericarditis should avoid physical activity until all symptoms have resolved and inflammatory markers have normalised. This is not a minor recommendation. Continuing to exercise while the pericardium is inflamed significantly increases the risk of complications.
Most children with straightforward viral pericarditis and small or no effusions manage treatment as outpatients with close follow-up. Admission becomes necessary when the effusion is large, when signs of cardiac tamponade are present, when bacterial pericarditis is suspected, or when the child is too unwell to be managed safely at home. This is a clinical judgement made case by case.
Inflammation of the pericardium often causes fluid to accumulate between the two layers of the sac. A small effusion is very common in acute pericarditis and in many cases resolves on its own as the inflammation settles.
The concern arises when the effusion becomes large. A large or rapidly accumulating effusion compresses the heart from outside, reducing its ability to fill and pump effectively. The echocardiogram determines the size of the effusion and its impact on cardiac function.
Cardiac tamponade is the condition in which a pericardial effusion has become large or rapid enough to interfere significantly with the heart's pumping function. Blood pressure falls, the heart beats faster to compensate, and in severe cases the child becomes gravely unwell.
Tamponade is a medical emergency. Pericardiocentesis, in which a needle drains the fluid from around the heart under ultrasound guidance, relieves the pressure immediately. Specialist cardiac centres perform this procedure in a catheterisation laboratory.
The majority of pericarditis cases in children do not progress to tamponade. The risk is higher with bacterial pericarditis, large effusions at presentation, and in children who have not received appropriate treatment early.
Recurrent pericarditis is the most common complication of the acute illness. Between 15 and 40 per cent of children who experience acute pericarditis will have at least one further episode. A recurrence is defined by the return of symptoms and diagnostic criteria after a symptom-free interval of at least four to six weeks.
Most recurrences can be managed with the same approach used for the initial episode: anti-inflammatory medication and colchicine. Colchicine is particularly important in reducing the frequency and severity of recurrences.
Specialists reserve corticosteroids for children whose pericarditis does not respond to NSAIDs (Ibuprofene) and colchicine, or when a specific autoimmune cause is identified. Their use requires careful specialist supervision because premature steroid use appears to increase the long-term risk of further recurrence.
Rilonacept and anakinra, interleukin-1 blocking agents, have emerged as effective options for children with multiple recurrences that do not respond to conventional treatment. These are specialist therapies prescribed in dedicated pericarditis clinics.
Dr Giardini reviews children with recurrent pericarditis at GOSH and in his private clinics in London, advising on tapering strategies, timing of colchicine withdrawal, and escalation when standard approaches prove insufficient. Experience matters here.
Constrictive pericarditis is a rare late complication in which the pericardium becomes thickened, scarred, and calcified following recurrent or prolonged inflammation. The rigid sac restricts the heart's ability to fill properly, producing a form of diastolic heart failure.
Children with constrictive pericarditis develop breathlessness, fatigue, reduced exercise tolerance, and abdominal swelling from raised venous pressure. The condition can be difficult to distinguish from restrictive cardiomyopathy on echocardiography alone, and cardiac MRI or cardiac catheterisation with pressure measurements is often needed for a definitive diagnosis.
Constrictive pericarditis requires surgical treatment. Pericardiectomy, in which surgeons remove the thickened pericardium, relieves the restriction and produces substantial improvement in most children. Outcomes are very good at experienced centres.
School attendance can usually resume once the child is comfortable, fever-free, and on appropriate treatment. Physically demanding activities and sport are a different matter.
Return to full physical activity, including school sport and any competitive training, should not happen until all symptoms have resolved, inflammatory markers have normalised, and the echocardiogram shows no effusion. Three to six weeks is typical. Competitive athletes may need a more formal exercise evaluation before returning to training.
These restrictions exist because physical stress on an inflamed pericardium can worsen the effusion and significantly increase the risk of recurrence. Guidance on return to sport for each child is provided individually at follow-up.
The outlook for most children with pericarditis is excellent. Viral and idiopathic pericarditis resolves completely in the majority, and the children involved go on to live entirely normal, active lives.
Recurrent pericarditis is frustrating but rarely life-limiting. With appropriate long-term management using colchicine and, where needed, newer anti-inflammatory agents, recurrences become less frequent and less severe over time. Most children eventually stop having episodes.
Constrictive pericarditis and cardiac tamponade are rare complications and both are treatable when identified appropriately. The factor that most influences outcome is how early the condition is recognised and how consistently treatment is followed in the initial episode.
How do I know if my child's chest pain could be pericarditis?
The most characteristic feature is pain that is clearly worse when lying flat and better when sitting forward or leaning slightly forward. This positional quality, combined with a recent viral illness, should prompt same-day medical assessment.
Is pericarditis dangerous in children?
Most cases are not. Viral pericarditis managed appropriately carries an excellent prognosis. The conditions that require urgent attention are large pericardial effusions and bacterial pericarditis. These are uncommon but need to be recognised and treated quickly.
Can my child go to school with pericarditis?
Once comfortable and afebrile, most children can return to school. Physical education and sport should be avoided until the inflammation has fully settled, which typically takes three to six weeks.
How long does pericarditis last in children?
An acute episode of viral pericarditis usually settles within two to four weeks with treatment. Some children have residual mild symptoms for longer. Treat recurrent episodes as new flares rather than concluding that the first episode failed to resolve.
What is the difference between pericarditis and myocarditis?
Pericarditis is inflammation of the sac surrounding the heart. Myocarditis is inflammation of the heart muscle itself. Both can produce chest pain and both can follow viral infections. They can occur together, which is called myopericarditis. Myocarditis typically produces more significant abnormalities of heart function and carries different treatment implications.
Can my child return to sport after pericarditis?
Yes, in time. Return to sport requires evidence that symptoms have fully resolved, inflammatory markers have normalised, and echocardiography shows no effusion. The typical minimum absence from competitive sport is three to six weeks, though this varies by individual.
Does pericarditis cause permanent heart damage?
In the vast majority of children, no. Viral and idiopathic pericarditis resolves completely without lasting cardiac effects. Constrictive pericarditis is a rare exception, but it is treatable surgically with good outcomes.
Why does my child's pericarditis keep coming back?
Recurrent pericarditis is common, affecting up to 40 per cent of children after a first episode. Colchicine significantly reduces recurrence risk. If episodes continue despite colchicine, specialist review is needed to consider underlying autoimmune causes and alternative treatments.
Should siblings be concerned if one child has pericarditis?
Viral pericarditis does not carry significant increased risk for siblings. When pericarditis is related to an autoimmune condition such as familial Mediterranean fever, there may be a genetic component worth discussing with a specialist.
When should I call 999 for pericarditis?
Call 999 if your child develops severe breathlessness at rest, appears grey or pale, feels faint, or the heart is racing alongside breathing difficulty. These features suggest cardiac tamponade, which requires emergency treatment.
Author: Dr. Alessandro Giardini, MD, PhD
Written 18/05/2026