
Dr. Alessandro Giardini
POTS is a syndrome (a combination of different symptoms) caused by a malfunction of the autonomic nervous system. The autonomic nervous system is a complicated network of nerves that controls some vital bodily functions and which works in an automatic mode out of our voluntary control. For example when we stand up quickly, we would all experience a slight drop of our blood pressure due largely to the effect of gravity and the body will have to enact some compensatory manoeuvres to re-establish a normal blood pressure. This will cause some of the body arteries and veins to shrink and the heart to start beating slightly stronger and faster. All this will happen in an automatic mode not under voluntary control.
The autonomic system controls many other systems in the body beside the heart rate and the size of the body arteries and veins. In some people the autonomic system may not work and leads to many of the symptoms observed in POTS.
.png)
Many conditions can affect the function of the autonomic system, thus producing “secondary” POTS. However, in some patients, a cause for POTS is not identified despite extensive investigation. POTS has been observed to commence after a viral infection, or an acute stress like surgery, a trauma or a vaccination. Many factors are also been associated with POTS and these include: physical deconditioning (being very unfit), excessive function of the adrenergic system (excessive release of adrenaline by the body), norepinephrine transporter deficiency, joint hyper mobility syndrome (Elhers-Danlos type III), chronic fatigue syndrome, and several autoimmune conditions.
Many parents notice that their child's symptoms began after what initially seemed like a straightforward viral illness. This is a well-recognised pattern, and one that comes up regularly in clinic. Children and teenagers may develop dizziness, palpitations, fatigue, chest discomfort, headaches, exercise intolerance, and concentration difficulties several weeks after recovering from infections including glandular fever, influenza, COVID-19, or other common viral illnesses.
The exact mechanism is not fully understood. Viral infections may temporarily disrupt autonomic nervous system regulation in susceptible individuals, affecting the normal control of heart rate and blood vessel tone during changes in posture. Recovery from the infection itself does not reset this dysregulation automatically. The heart racing when standing up, a teenager feeling dizzy after standing, or a child feeling faint standing up in the weeks following a viral illness are all patterns worth taking seriously.
This does not mean the infection is still active. Rather, the autonomic system has become dysregulated in the wake of the acute illness, and recovery from that dysregulation follows its own timeline.
Post-viral PoTS is not a new concept, though awareness increased substantially following the COVID-19 pandemic. A formal assessment, including the active standing test and cardiac investigations, establishes the diagnosis clearly and distinguishes post-viral PoTS from other possible explanations. Dr Giardini takes a detailed history of any preceding illness when assessing children with a new presentation of autonomic symptoms, because the timing and trigger frequently inform both the diagnosis and the management plan.
I assess and manage children and adolescents with dizziness, fainting, orthostatic intolerance and POTS in my London clinics and at Great Ormond Street Hospital.
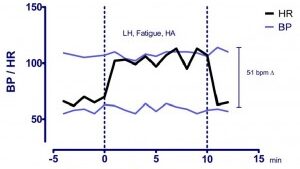
To be diagnosed with POTS children and adults have to have a combination of symptoms (not necessarily all symptoms) which occur when they are in the upright position (generally when standing) which improves or resolve when lying down. Besides the typical symptoms, it is necessary to document an abnormal function of the component of the autonomic system that controls heart rate. In practical terms this is done by measuring the change in heart rate observed from lying down to standing up. A sustained increase in heart rate of >40 beats minute in the 10 minutes following standing is considered diagnostic in children. An absolute increase in the heart rate above 120 beats/minute is also considered diagnostic. Blood pressure can drop while standing in patients with POTS but there should beno drop of the systolic blood pressure of more than 20 mmHg and no drop in the diastolic blood pressure of more than 10 mmHg. This test (called an active standing test) can be performed on an outpatient basis.
Additional tests are required to ensure that the symptoms are not due to a cardiac or neurologic problem as many cardiac or neurologic conditions can produce very similar symptoms to POTS.
Excluding a cardiac cause for the symptoms (an arrhythmia or a structural heart problem) generally requires seeing a cardiologist with expertise in POTS as well as undertaking an electrocardiogram (ECG) and an echocardiogram. In some instances further tests may be required (24 hour ECG monitoring, active standing test, head up tilt test, cardiac MRI). Additionally blood tests will also be required at the time of the assessment.
The symptoms of POTS are numerous and can be very disabling. This is particularly true as most of the usual cardiology investigations and tests performed in children and adults with POTS will be usually reported as normal despite patients objectively reporting the heart rate as being excessively high and the heart pounding (palpitations). Additionally many physicians are unaware of POTS.
The most common symptoms noted in POTS are:
Some triggers are known to worsen symptoms:
Many children and teenagers with PoTS describe feeling persistently unwell despite most medical tests coming back completely normal. That gap between how much a child suffers and how reassuring the test results appear is one of the most distressing aspects of the condition for families.
Standing is where things most commonly fall apart. Teenagers frequently describe dizziness in the shower, struggling to stand still in queues or school assemblies, and a racing heartbeat after climbing a single flight of stairs. Brain fog, commonly described as difficulty thinking clearly or following lessons, affects many young people during the school day regardless of how much they have slept. Nausea and abdominal discomfort are also more common in PoTS than many parents expect, and they can be as disabling as the cardiovascular symptoms.
Mornings are typically the hardest part of the day. Blood circulation regulation tends to be least stable shortly after waking, compounded by overnight dehydration. Many children feel at their worst for the first one to two hours after getting up, which significantly affects school attendance and morning routines. That pattern, much worse on rising and gradually better as the day progresses, is one of the first things Dr Giardini asks about in the clinical assessment.
Symptoms fluctuate considerably from day to day. Good days can give false reassurance that the problem has resolved, only for symptoms to return during heat, illness, physical activity, or a stressful period. One important feature of PoTS is that symptoms are typically worse upright and improve, at least partially, when lying down. That positional quality is one of the most diagnostically informative features of the condition.
Many families become frustrated that their child appears outwardly healthy while describing significant limitations in daily life. That frustration is entirely understandable, and it does not mean the symptoms are exaggerated. The heart rate data, when formally measured on the active standing test, usually makes the clinical picture unmistakably clear.
The diagnosis of PoTS in children and adolescents is based on a combination of the clinical history and a documented abnormal heart rate response to standing. The key test is called an active standing test. The child lies flat for at least ten minutes while heart rate and blood pressure are recorded, and then stands up quickly and remains standing for a further ten minutes. A sustained increase in heart rate of 40 beats per minute or more within those ten minutes, in the absence of a significant drop in blood pressure, is considered diagnostic. An overall and persistent increase in the heart rate above 120 beats/minute in the 10 minutes of standing is also an accepted criteria for the diagnosis. This test is simple, painless, and can be performed in the outpatient clinic. In cases where the diagnosis remains uncertain, a head-up tilt table test provides a more controlled assessment: the child is secured to a table that is tilted to a near-upright position while heart rate, blood pressure, and symptoms are monitored continuously. An ECG is essential to rule out arrhythmias or electrical abnormalities that might mimic PoTS symptoms. An echocardiogram is performed when there is any clinical suspicion of structural heart disease, an abnormal cardiac examination, or a relevant family history. Blood tests are used to exclude contributing conditions such as thyroid dysfunction, iron deficiency anaemia, and vitamin D deficiency. In selected cases, a 24-hour Holter monitor or a cardiopulmonary exercise test may be added to complete the picture. Dr Giardini performs the active standing test, ECG, and echocardiogram together as part of a single appointment, allowing a clear diagnosis and management plan to be established on the same day.
Many of the symptoms of POTS can improved with a multidisciplinary approach which includes lifestyle changes, counter maneuvers, physiotherapy/exercise and medications. Medications include those that slow down the excessive increase of heart rate (ivabradine or beta-receptors blockers), those that increase blood pressure (midodrine) and those which expand blood volume (fluidrocortisone). Medications are generally used to get children well enough to be able to start a physiotherapy/rehabilitation program. The majority of children who develop POTS as adolescents will not have symptoms by the time they will be young adults.
The outlook for adolescents with PoTS is generally good. Symptoms can be genuinely disabling during the teenage years, and families often face a difficult period before the right management plan is established. Most children improve substantially over time, particularly when a structured approach combining adequate hydration, salt supplementation, graded exercise reconditioning, sleep optimisation, and medication where needed is followed consistently.
Recovery is rarely a straight line. Good weeks are often followed by setbacks, particularly during viral illnesses, growth spurts, stressful academic periods, and hot weather. Families who understand that fluctuation is a normal part of recovery tend to cope considerably better than those expecting steady, uninterrupted improvement. The great majority of children who develop PoTS in adolescence no longer have significant symptoms by their early twenties.
Yes. Chest discomfort is common in PoTS and is usually related to autonomic dysfunction, the rapid heart rate itself, or overactivation of the chest wall muscles during postural changes. A thorough assessment including an ECG and echocardiogram confirms that the heart is structurally normal and allows the symptom to be properly understood in context.
Blood circulation regulation is typically least stable shortly after waking, particularly following overnight dehydration. Starting the day with fluid intake before standing, and rising gradually from a seated position, helps reduce the severity of morning symptoms in many children.
Yes, and significantly so in some children. Fatigue, dizziness, headaches, and concentration difficulties can make a full school day extremely challenging. Dr Giardini provides written school guidance letters where appropriate, which help teachers and pastoral staff understand what reasonable adjustments look like without restricting a child more than necessary.
Most adolescents with PoTS improve substantially over time, and many no longer have significant symptoms by early adulthood. This does not mean watchful waiting is the only approach. Structured rehabilitation and targeted treatment significantly speed recovery and reduce the impact on daily teenage life during that period.
Anxiety does not cause PoTS. The two conditions can overlap, and anxiety commonly worsens autonomic symptoms, but the underlying autonomic dysfunction in PoTS is a distinct physiological finding, not a psychological one. Many children with PoTS are initially, and incorrectly, told their symptoms are solely anxiety-related. Formal assessment provides the clarity families need.
PoTS can be very disabling and significantly affects quality of life, but it is not usually life-threatening in children and teenagers. The main importance of proper specialist assessment is ruling out other cardiac conditions that can produce similar symptoms but carry different implications for management and safety.
Exercise is one of the most effective long-term treatments for PoTS, but it must be introduced gradually and structured carefully. Poorly timed or excessive exercise early in the recovery process can temporarily worsen symptoms. A physiotherapist experienced in autonomic conditions works best alongside the cardiologist in guiding this programme, and Dr Giardini can advise on referral pathways.
Joint hypermobility is commonly associated with PoTS in teenagers, and this relationship is well established in the published literature. Children who have hypermobile joints alongside PoTS symptoms benefit from assessment that addresses both dimensions. Dr Giardini takes a detailed musculoskeletal history as part of the standard PoTS evaluation.
Author: Dr. Alessandro Giardini, MD, PhD
Written 26/05/2026