
Dr. Alessandro Giardini
.png)
If you have been told that your child has a patent ductus arteriosus, it is completely natural to feel concerned. The reassuring news is that PDA is a common and well-understood condition, particularly in newborn babies, and the overall outlook is excellent. Many small PDAs close on their own in the first weeks of life without any treatment at all. When closure is needed, it can almost always be achieved safely and effectively, and most children go on to lead completely normal, active lives.
Before birth, every baby has a blood vessel called the ductus arteriosus. This vessel connects the pulmonary artery (which leads to the lungs) to the aorta (the main artery carrying blood to the body). During pregnancy, the baby receives oxygen directly from the mother's placenta, so the lungs are not yet in use. The ductus arteriosus allows blood to bypass the lungs and flow straight to the body, which is exactly what is needed at this stage of development.
After birth, as the baby takes its first breaths and the lungs begin to work, this vessel is no longer required. In most babies, the ductus arteriosus closes naturally within the first two to three days of life. A patent ductus arteriosus means that this vessel has remained open.
When the ductus stays open, some oxygen-rich blood from the aorta flows back through the vessel into the pulmonary artery and returns to the lungs unnecessarily. This results in extra blood flowing through the lungs and increased workload on the left side of the heart, which has to pump harder to compensate. The significance of this depends on the size of the PDA. A tiny ductus may cause no problems whatsoever, while a large one can place considerable strain on the heart and lungs.
It is worth knowing that in some babies born with certain complex congenital heart defects, the PDA actually plays a helpful role by maintaining blood flow to the lungs or the body. In these cases, doctors may give medication to keep the ductus open deliberately. This is a very different situation from the isolated PDA described on this page.
In most cases, there is no clear cause. The ductus simply does not close as expected after birth. PDA is significantly more common in premature babies, because the normal physiological signals that trigger closure of the duct are less well developed in babies born early. Studies suggest that PDA affects around 65% of infants born before 28 weeks of pregnancy, while it is much less common in full-term babies.
PDA is approximately twice as common in girls as in boys. Other factors that may increase the risk include low birth weight, neonatal respiratory distress syndrome, genetic conditions such as Down syndrome, and maternal rubella (German measles) infection during pregnancy. However, in the majority of full-term babies with a PDA, no specific risk factor is identified.
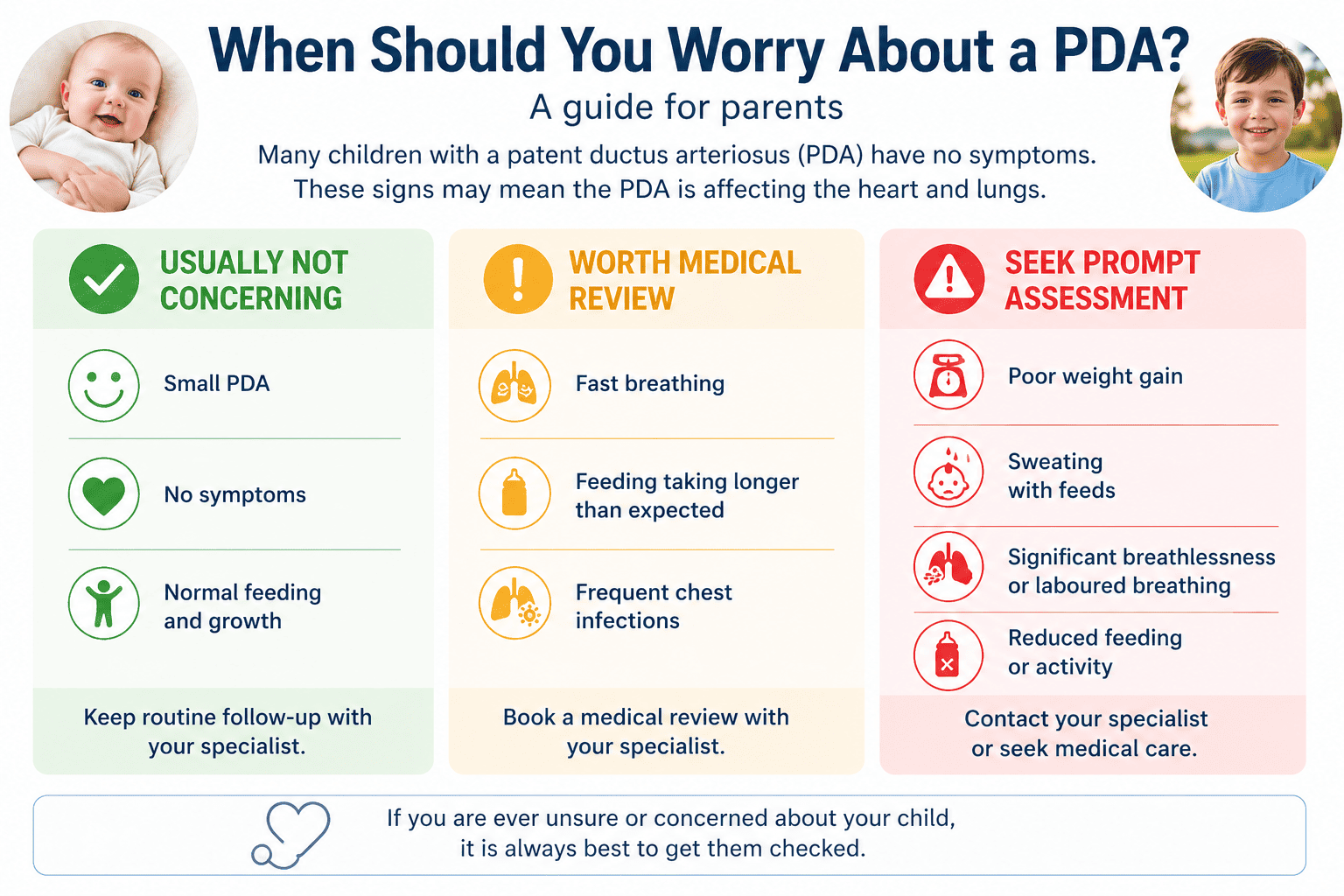
Many children with a PDA have no symptoms at all, particularly when the ductus is small. In these cases, the PDA is often discovered incidentally when a doctor hears a characteristic heart murmur during a routine examination. The murmur associated with a PDA is often described as "continuous" or "machinery-like" because it can be heard throughout both the heartbeat and the pause between beats. This distinctive sound frequently provides the first clue to the diagnosis.
When a PDA is moderate or large, symptoms arise because of the extra blood flowing through the lungs and the increased work the heart has to do. In babies, these symptoms may include fast or laboured breathing, difficulty feeding or tiring during feeds, sweating during feeding, poor weight gain and frequent chest infections. Premature infants with immature lungs are particularly sensitive to the extra pulmonary blood flow and may develop breathing difficulties requiring ventilator support.
Symptoms in babies with a large PDA typically become apparent in the first weeks of life. Older children with a PDA that has not been treated may notice breathlessness during physical activity and reduced exercise tolerance compared to their peers, although this presentation is uncommon because most significant PDAs are identified and managed much earlier.
🟢 Usually not concerning
🟡 Worth medical review
🔴 Seek prompt assessment
In full-term infants, a PDA is most often first suspected when a doctor hears the characteristic continuous murmur during a routine examination. In premature babies, the murmur may be less distinct, and the diagnosis may be suspected when a baby develops unexplained breathing difficulties soon after birth.
The key diagnostic test is an echocardiogram, a painless ultrasound scan of the heart. This allows Dr Giardini to confirm the presence of the PDA, assess its size and shape, measure how much blood is flowing through it, and evaluate whether the left side of the heart has become enlarged from handling the extra volume. Dr Giardini performs and interprets all echocardiograms personally, so findings can be discussed with you immediately.
An electrocardiogram (ECG) and chest X-ray may also be performed. In babies with a large PDA, the chest X-ray may show an enlarged heart and increased blood flow to the lungs. In most cases, however, the echocardiogram provides all the information needed to guide management.
Not always. Many small PDAs cause no haemodynamic problems and simply need periodic monitoring. Some close on their own during the first year of life without any intervention.
Treatment is considered when the PDA is large enough to cause symptoms, when there is evidence of increased strain on the heart, or when the baby is failing to grow adequately. In older children with a small but audible PDA that has not closed, closure may also be recommended to eliminate the risk of endocarditis, a serious infection of the heart lining that can be caused by turbulent blood flow through the open duct. When a small PDA is truly "silent" (causing no murmur and found incidentally on a scan), treatment is generally not required.
The aim of treatment is always to close the PDA, stop the abnormal blood flow and allow the heart and lungs to return to normal function.
The approach depends on the baby's age, weight and clinical condition, as well as the size of the PDA.
Medical treatment is most commonly used in premature babies. Medications such as ibuprofen or indomethacin (non-steroidal anti-inflammatory drugs) can encourage the ductus to close by blocking the prostaglandins that help keep it open. These medications are most effective when given within the first ten days after birth and work better in premature infants than in full-term babies. Several doses may be needed. If the ductus does not respond to medication, a procedural or surgical approach is considered.
Catheter-based closure is the most common treatment for PDAs in older infants and children and has become the preferred approach at most specialist centres. The procedure is performed under sedation or general anaesthetic. A thin, flexible catheter is inserted into a blood vessel in the leg and guided up to the ductus arteriosus. A small coil or plug-shaped closure device is then positioned within the ductus to block the blood flow permanently. The choice between a coil (for smaller PDAs) and a plug device (for larger ones) depends on the size and shape of the ductus. The procedure is minimally invasive, avoids the need for open surgery, typically requires only an overnight hospital stay, and results are excellent. Blood flow returns to normal immediately after successful closure.
Surgical closure is reserved for very small premature babies in whom catheter-based closure is not technically feasible, for babies with very large PDAs, or when the anatomy is unusual. The surgeon closes the ductus through a small incision on the left side of the chest, using stitches or a metal clip. The operation does not require a heart-lung bypass machine. Recovery is usually straightforward, and the results are very good.
Children with a PDA have a small but recognised risk of developing endocarditis, an infection of the inner lining of the heart or blood vessels caused by bacteria entering the bloodstream. The turbulent blood flow through an open ductus makes the area more susceptible to infection. Good dental hygiene, including regular brushing, flossing and routine dental visits, is the most important way to reduce this risk. According to current guidelines, most children with a PDA do not require routine antibiotics before dental procedures, although this may be recommended for the first six months after closure. The endocarditis risk is one reason why closure of even a small but audible PDA is sometimes recommended.
A small, silent PDA generally poses no long-term risk. However, larger untreated PDAs can cause progressive damage over time. The sustained extra blood flow through the lungs can lead to pulmonary hypertension (high pressure in the lung blood vessels), which may eventually damage the lung vasculature permanently. Untreated large PDAs can also cause enlargement and weakening of the heart, leading to heart failure. In rare, long-standing cases, irreversible lung damage known as pulmonary vascular disease can develop. This is why timely assessment and, when indicated, early closure are important.
The outlook for children with a PDA is excellent. Many small PDAs close spontaneously in the first weeks or months of life. Those that require treatment, whether by medication, catheter device or surgery, are almost always corrected successfully. Full-term children who have their PDA closed and have no other heart defects can expect normal activity levels, normal growth and a normal lifespan. Once a PDA has been closed, long-term follow-up is usually minimal unless there are other cardiac concerns.
For premature babies, the outlook after PDA treatment depends partly on other factors related to prematurity, such as lung development and overall growth. Dr Giardini will discuss your child's individual situation and any ongoing follow-up that may be needed.
If you have any concerns about your child or would like to arrange an assessment, please do not hesitate to contact Dr Giardini's team to book an appointment.
Most PDAs are not dangerous, particularly when they are small. Larger PDAs may need treatment to prevent strain on the heart and lungs, but outcomes after closure are excellent.
Yes. Many PDAs close naturally in the first days or weeks of life. If a PDA has not closed by the age of one to two years, it is unlikely to do so on its own, and closure may be recommended.
Yes. Premature babies are significantly more likely to have a PDA because the normal closure mechanism is less mature. The earlier the baby is born, the higher the likelihood.
In babies, the most important signs are fast or laboured breathing, difficulty feeding, sweating during feeds, poor weight gain and frequent chest infections.
In most cases, no. The majority of PDAs that need treatment can be closed using a catheter-based procedure, which is minimally invasive and avoids open surgery. Surgery is only needed in selected cases, such as very small premature babies.
Ibuprofen or indomethacin can be given to premature babies to encourage the ductus to close. These medications are most effective in the first ten days after birth and may require several doses.
A thin tube is inserted through a blood vessel in the leg and guided to the heart. A small coil or plug device is positioned within the ductus to seal it permanently. The procedure usually requires only an overnight hospital stay.
Yes. Most children who have their PDA closed lead completely normal, active lives with no restrictions on physical activity.
In most cases, routine antibiotic prophylaxis is not required. It may be recommended for the first six months after PDA closure. Good dental hygiene is the most effective way to prevent endocarditis.
When should I see a specialist?
If your child has been diagnosed with a PDA, or if a heart murmur has been detected, specialist assessment with Dr Giardini is recommended to determine the significance of the PDA and advise on whether monitoring or treatment is needed.
Author: Dr. Alessandro Giardini, MD, PhD
Written 03/05/2026