
Dr. Alessandro Giardini
.png)
If you have been told that your child has a problem with the aortic valve, it is natural to feel concerned. The reassuring starting point is this: many children with aortic valve conditions are well, active and living completely normal lives, particularly when the problem is mild. When treatment is needed, it is usually planned carefully rather than done urgently, and outcomes are very good.
A key part of specialist assessment is understanding how severe the valve problem is and whether your child needs monitoring or treatment. Dr Giardini regularly assesses children with aortic valve conditions and can provide this clarity during a single appointment.
The aortic valve sits between the left ventricle (the heart's main pumping chamber) and the aorta, the large artery that carries oxygen-rich blood to the body. A normal aortic valve has three thin leaflets that open fully with each heartbeat and close tightly between beats.
Aortic stenosis means the valve is narrowed and does not open fully, forcing the left ventricle to work harder. Over time, this extra workload causes the heart muscle to thicken.
Aortic regurgitation (also called a leaky aortic valve) means the valve does not close properly, allowing blood to leak backwards into the left ventricle. The heart has to pump this extra blood forward again, which can cause the left ventricle to enlarge over time.
Many children have a combination of both, particularly when the underlying problem is a bicuspid aortic valve.
The most common cause is a congenital abnormality of the valve present from birth. A bicuspid aortic valve, where the valve has two leaflets instead of the normal three, is the single most frequent underlying finding, affecting approximately 1 to 2% of the population. While many bicuspid valves function normally for years, they are more prone to developing stenosis, regurgitation or both over time.
Other congenital causes include thickened or fused valve leaflets, an unusually small valve, and narrowing below the valve (sub-valvular stenosis, often caused by a fibrous ridge) or above it (supra-valvular stenosis, associated with Williams syndrome). Identifying the exact level of obstruction is important because it affects the treatment approach.
Less commonly in the UK, aortic valve damage can be acquired after rheumatic fever. In most cases, nothing a parent did or did not do caused the valve abnormality.
Many children with mild or moderate aortic stenosis or regurgitation have no symptoms at all. They feel entirely well, grow normally, are fully active, and the condition is often discovered only because a doctor hears a heart murmur or an ejection click during a routine examination.
When symptoms do occur, they usually reflect more significant valve dysfunction and may include reduced exercise tolerance, breathlessness during physical activity, chest discomfort or tightness on exertion, dizziness or lightheadedness, palpitations, and unusual fatigue. Fainting during exercise in a child with known aortic valve disease is an important warning sign that should always prompt urgent specialist review, as it may indicate severe obstruction.
In babies with critical aortic stenosis, the presentation can be very different. Critical stenosis in the newborn period is a serious condition in which the valve is so severely narrowed that the heart cannot pump enough blood to the body. Babies may present in the first days of life with poor feeding, rapid breathing, pallor, lethargy and signs of heart failure. This is a medical emergency requiring immediate treatment. Prostaglandin E1 is given intravenously to keep the ductus arteriosus open and maintain blood flow to the body while urgent intervention is arranged.
Parents should understand that the absence of symptoms in a child with known aortic valve disease is reassuring but does not eliminate the need for regular follow-up. Some changes develop gradually and can be detected on echocardiography before they cause any symptoms, which is precisely why monitoring matters.
Most children are first suspected to have an aortic valve problem when a heart murmur is heard during a routine examination. The murmur of aortic stenosis is typically a harsh, ejection-type sound heard at the upper right side of the chest and sometimes radiating to the neck. An ejection click, a brief sharp sound at the moment the valve opens, may also be heard and is characteristic of a bicuspid valve. The murmur of aortic regurgitation is a softer, blowing sound heard along the left side of the breastbone.
The key diagnostic test is an echocardiogram, a painless ultrasound scan of the heart. Dr Giardini performs and interprets all echocardiograms personally, providing a detailed assessment of the valve structure, the number of leaflets, the degree of stenosis (measured by the pressure gradient across the valve), the severity of any regurgitation, the thickness and function of the left ventricle, and the dimensions of the aorta. Results are available immediately and can be discussed during the same appointment.
An electrocardiogram (ECG) is usually performed to check for signs of left ventricular thickening. In older children and adolescents, an exercise test may be valuable for assessing how the heart responds to physical stress and for unmasking symptoms that are not apparent at rest. Cardiac MRI is used when more detailed assessment of valve function, ventricular volumes or aortic dimensions is needed, and is particularly helpful for planning treatment.
Not always, and this is often the most reassuring part of the consultation. The decision depends on the severity of the stenosis or regurgitation, whether the heart is showing signs of strain, and whether the child has symptoms.
Mild aortic stenosis or regurgitation typically requires monitoring only. Many children remain in this category for years or even indefinitely, with periodic echocardiograms to confirm that the valve and the heart remain stable.
Moderate disease warrants closer follow-up. Some children with moderate stenosis or regurgitation remain stable for a long time, while others may gradually progress and eventually require treatment. Regular assessment allows Dr Giardini to track the trajectory and plan any intervention at the optimal time.
Severe aortic stenosis or regurgitation generally requires treatment, particularly when there is evidence of left ventricular thickening (in stenosis), left ventricular enlargement (in regurgitation), or when symptoms are present. The aim is to relieve the obstruction or correct the leak before the heart is permanently affected.
It is important for parents to understand that all treatments for aortic valve disease in children are aimed at improving or correcting the valve problem, but they do not create a normal valve. This is why lifelong follow-up with a cardiologist is essential, even after successful treatment.
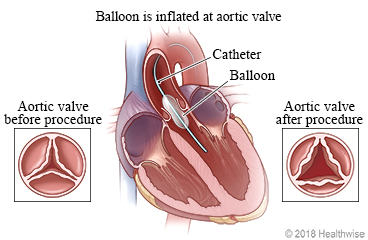
The most common initial treatment for significant aortic stenosis is balloon aortic valvuloplasty. A thin catheter with a deflated balloon at its tip is inserted through a blood vessel (usually in the leg, or through the umbilical vessels in newborns) and guided to the aortic valve. The balloon is inflated briefly to stretch the narrowed valve open, then removed. The procedure avoids open-heart surgery, requires only a short hospital stay, and is effective at reducing the obstruction in the majority of children.
Balloon valvuloplasty does not make the valve normal. It may leave some residual stenosis or cause a degree of regurgitation. Published data show it is associated with a higher rate of reintervention over the following 10 years compared with surgical valvotomy, but it remains the preferred first-line treatment because it is less invasive and preserves the native valve for as long as possible.
When balloon valvuloplasty is not effective, when the valve anatomy is not suitable for balloon treatment, or when the stenosis recurs, surgical options are considered. These include surgical valvotomy (direct opening of the fused valve leaflets under direct vision), valve repair (reconstruction of the leaflets to improve function), and valve replacement.
Mild aortic regurgitation often requires no treatment at all and is simply monitored with periodic echocardiography. Many children remain stable with mild regurgitation for years.
When regurgitation is more significant and the left ventricle begins to enlarge or its function starts to decline, treatment is recommended. The timing of intervention for aortic regurgitation requires careful judgement, because operating too early exposes the child to unnecessary surgical risk, while waiting too long may allow irreversible changes to develop in the heart muscle.
Aortic valve repair, where the surgeon reconstructs the existing valve leaflets to improve closure, is the preferred approach when the anatomy is favourable. Repair preserves the child's own tissue and avoids the need for anticoagulation medication.
When repair is not feasible, valve replacement becomes necessary. The options for valve replacement in children include the Ross procedure, mechanical valve replacement and biological (tissue) valve replacement.
The Ross procedure is uniquely suited to children and young people. The child's own pulmonary valve is transplanted into the aortic position, and a donor valve (homograft) is placed in the pulmonary position. The key advantage is that the pulmonary autograft is a living valve that grows with the child, avoids lifelong anticoagulation, and has been shown to restore life expectancy to that of the general population. Published paediatric series report 10-year survival of approximately 93% with excellent functional outcomes.
.jpg)
The main long-term consideration is that the autograft can gradually dilate over time, potentially leading to recurrent regurgitation, though modern reinforcement techniques have significantly reduced this risk. The homograft may also require replacement as the child grows, although transcatheter techniques increasingly allow this without open-heart surgery.
Mechanical valve replacement provides a durable valve that rarely wears out but requires lifelong anticoagulation with warfarin, with regular blood testing to ensure the correct dose. This carries a small ongoing risk of bleeding or blood clots. For older adolescents and young adults who can manage anticoagulation reliably, a mechanical valve can be an appropriate choice.
Biological (tissue) valve replacement avoids the need for anticoagulation but has limited durability, particularly in children and young people whose active circulation wears the valve out more quickly than in older adults. Most biological valves in children will need replacing within 10 to 15 years.
The choice between these options is highly individualised and depends on the child's age, anatomy, lifestyle and family preferences. Dr Giardini will discuss the advantages and limitations of each approach clearly if valve replacement becomes necessary.
Not all aortic obstruction occurs at the valve itself. Sub-valvular aortic stenosis is caused by a fibrous ridge or membrane that grows just below the aortic valve in the left ventricular outflow tract. It can develop gradually during childhood and may not be present at the initial diagnosis. Sub-valvular stenosis does not respond to balloon dilatation and requires surgical removal if it becomes significant. It has a tendency to recur after surgery, which is why ongoing monitoring is important.
Supra-valvular aortic stenosis is a narrowing of the aorta just above the valve. It is characteristically associated with Williams syndrome, a genetic condition, but can also occur in isolation. Treatment, when needed, is surgical.
For most children with mild aortic valve disease, the answer is yes. Children with mild stenosis or regurgitation and normal heart function can participate fully in sport without restriction.
Children with moderate disease need individualised advice, and high-intensity competitive sport or heavy weightlifting may be restricted. Children with severe aortic stenosis should avoid strenuous exercise until treated, because of the small but recognised risk of serious cardiac events during intense exertion. After successful treatment, most children return to an active lifestyle. Dr Giardini provides individualised exercise guidance based on each child's specific findings.
The long-term outlook for children with aortic valve disease is good, though this is typically a lifelong condition requiring ongoing follow-up. Stenosis can slowly worsen, regurgitation can increase, and valves that have been treated may eventually require further intervention as the child grows.
The key to the best outcome is early diagnosis, appropriate timing of treatment, and consistent lifelong follow-up. With modern techniques, most children who need treatment do very well and grow into healthy, active adults. If you are concerned about your child's aortic valve, Dr Giardini can provide a same-day echocardiogram and a clear explanation of what the findings mean. Please do not hesitate to contact his team to arrange an appointment.
It depends on the severity. Mild aortic stenosis or regurgitation is usually harmless and simply needs monitoring. Moderate disease requires careful follow-up. Severe disease can place strain on the heart and requires treatment, but outcomes with modern techniques are very good.
Aortic valve conditions do not typically resolve on their own. Mild cases may remain stable for many years, but because progression is possible, lifelong monitoring with periodic echocardiography is recommended.
Not always. Many children with aortic valve disease are managed with monitoring alone. When treatment is needed, the first approach is often balloon valvuloplasty, which avoids open-heart surgery. Surgical valve repair or replacement is reserved for cases that are more severe or that do not respond to catheter-based treatment.
The Ross procedure replaces the diseased aortic valve with the child's own pulmonary valve, which is a living valve that grows with the child and avoids the need for lifelong anticoagulation. It is the only aortic valve replacement that has been shown to restore life expectancy to that of the general population.
In most cases, yes. Children with mild disease and normal heart function can participate fully in sport. Those with moderate or severe disease need individualised advice. Dr Giardini provides specific exercise guidance based on each child's valve function and cardiac assessment.
Stenosis means the valve is narrowed and does not open fully, making the heart work harder to pump blood through it. Regurgitation means the valve does not close properly, allowing blood to leak backwards. Some children have both.
This depends on the severity. Children with mild, stable disease may need echocardiograms every one to two years. Those with moderate or progressive disease are reviewed more frequently. Dr Giardini will set an individualised follow-up plan.
The most common underlying cause, bicuspid aortic valve, has a recognised genetic component. First-degree relatives (parents and siblings) of a child with a bicuspid aortic valve are recommended to have a screening echocardiogram, even if they have no symptoms.
Critical aortic stenosis is a severe narrowing of the aortic valve that presents in the first days of life. It is a medical emergency requiring urgent treatment, usually with prostaglandin medication to maintain blood flow followed by balloon valvuloplasty.
If a heart murmur has been detected, if your child has symptoms during exercise, if there is a known valve problem, or if you simply want reassurance, a specialist assessment with Dr Giardini can provide a definitive answer. The echocardiogram and results are completed in a single appointment, so families do not face an extended wait for answers.
Author: Dr. Alessandro Giardini, MD, PhD
Written 03/04/2026