
Dr. Alessandro Giardini
If you have been told that your child has a "hole in the heart," it is completely natural to feel worried. The reassuring news is that an atrial septal defect (ASD) is one of the most common congenital heart conditions, and the outlook for children diagnosed with one is excellent. Many small defects cause no problems at all and close on their own, while those that do require treatment can almost always be corrected with a straightforward procedure.
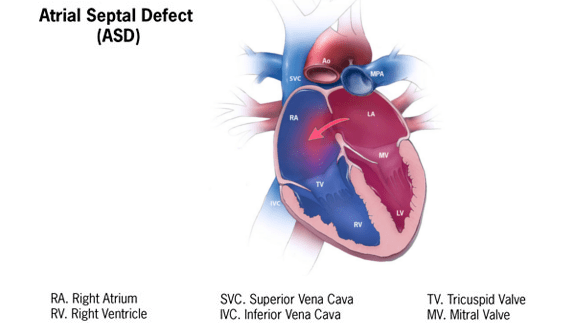
The heart has four chambers. The two upper chambers are called the atria and they are separated by a thin wall known as the atrial septum. An atrial septal defect is a gap in this wall that allows blood to pass between the left and right atrium.
In a normal heart, oxygen-rich blood returns from the lungs to the left atrium and is pumped out to the body, while oxygen-poor blood returns to the right atrium and is sent to the lungs. With an ASD, some oxygen-rich blood from the left atrium flows back across the hole into the right atrium instead of going out to the body. This means the right side of the heart handles more blood than it should, and more blood than necessary flows through the lungs. The significance of this extra flow depends almost entirely on the size of the defect.
It is worth noting that a small opening between the atria is actually normal before birth. This opening, called the patent foramen ovale (PFO), helps blood circulate while the baby is in the womb and usually closes naturally in the weeks after delivery. A PFO is not the same as a true ASD and is generally considered a normal finding in infancy. Dr Giardini can explain the difference clearly if this distinction arises during your child's assessment.
.png)
In the vast majority of cases, there is no identifiable cause. ASDs develop during the early weeks of pregnancy when the heart is forming, and in most children nothing a parent did or did not do played any role. ASDs can occasionally run in families and are slightly more common in girls than boys. In a small number of cases, an ASD may be associated with a genetic condition (like Holt-Oram syndrome), but most occur as isolated findings in otherwise healthy children.
There are several types, classified by where on the atrial septum the defect is located. The ostium secundum ASD is the most common, accounting for the large majority of cases. It occurs in the central portion of the septum and is the type most suitable for catheter-based (keyhole) closure. Other types include the ostium primum ASD, which sits in the lower part of the septum close to the heart valves, the sinus venosus ASD, which occurs near the entry of the large veins into the atrium, and the rare coronary sinus defect. The type of ASD matters because it determines which treatment approach is most appropriate if closure is needed. Dr Giardini will explain your child's specific anatomy during the consultation.
Most children with an ASD have no symptoms at all, and this is an important point for parents to understand. Many defects are discovered incidentally when a doctor hears a heart murmur during a routine examination or when a scan is performed for an unrelated reason.
When symptoms do occur, they tend to develop gradually and may include becoming tired more easily than other children, mild breathlessness during physical activity, frequent chest infections, or, in babies, slower feeding or poor weight gain. These symptoms are more likely when the defect is large enough to cause significant extra blood flow to the right side of the heart.
🟢 Usually not concerning:
- No symptoms
- Small defect on scan
- Normal growth and activity
🟡 Worth medical review:
- Getting tired more easily than peers
- Frequent chest infections
- Shortness of breath with activity
🔴 Seek prompt assessment:
- Poor weight gain in babies
- Significant breathlessness
- Palpitations or fainting in older children
.png)
The key investigation is an echocardiogram, a painless ultrasound scan of the heart. This allows Dr Giardini to see the defect directly, measure its size, assess how much blood is crossing from left to right, and determine whether the right side of the heart has become enlarged. Dr Giardini performs and interprets all echocardiograms personally, so findings can be discussed with you immediately during the same appointment.
An electrocardiogram (ECG) is usually performed alongside the echocardiogram to check the heart's electrical activity and provide additional information about how the right side of the heart is coping. In some older children, further tests such as a cardiac MRI or an exercise test may be helpful to assess heart function more precisely, but in most cases the echocardiogram provides all the information needed.
A key part of Dr Giardini's consultation is explaining clearly whether the defect is something to monitor or something that may benefit from treatment, and importantly, when any decision needs to be made.
Not always. The decision depends on several factors: the size of the defect, how much extra blood is flowing through it, whether the right side of the heart is showing signs of enlargement, and whether your child has any symptoms.
Many small ASDs cause no haemodynamic problems at all. These defects are simply monitored with periodic echocardiograms, and a significant proportion of secundum ASDs close spontaneously during childhood without any intervention. When the defect is larger, it can allow enough extra blood to flow through the right side of the heart that, over time, the right chambers may enlarge and the lungs may come under increased strain. In these situations, closing the defect is usually recommended to prevent long-term complications.
The important point for parents is that treatment is rarely urgent. Decisions are made carefully, based on how your child is doing over time rather than at a single appointment. In many children, closure is planned electively during early childhood, typically between the ages of three and six, allowing time to see whether the defect will close on its own. Some children with large ASD may however develop significant heart dilatation and symptoms in the first of life and these children may benefit from early closure of the defect, usually trough cardiac surgery.
When closure is needed, the most common approach is transcatheter (keyhole) device closure. This is performed in a catheterisation laboratory under general anaesthetic. A thin, flexible tube (catheter) is inserted through a vein in the leg and guided to the heart. A small closure device is then positioned across the hole, where it sits against the septum on both sides and seals the defect. Over time, the heart's own tissue grows over the device, incorporating it permanently. The procedure avoids open-heart surgery, typically requires only an overnight hospital stay, and most children return to normal activities within a few days. Published data from large multicentre studies confirm that transcatheter ASD closure in children has a success rate above 95% and a very low complication rate.
After the procedure, children usually take a low dose of aspirin for around six months while the device becomes fully covered by the heart's own tissue. Dr Giardini will arrange follow-up echocardiograms to confirm that the device is well positioned and the defect is fully closed.
Surgical closure is needed in a smaller number of cases where the anatomy is not suitable for a device, for example when the defect is very large, when the surrounding tissue rims are insufficient to anchor a device securely, or when the ASD is a type other than secundum. Surgery involves closing the hole with stitches or a small patch through an incision in the chest, and outcomes are excellent. Most children spend three to four days in hospital and recover fully within about six weeks.
Small ASDs that do not cause right heart enlargement generally pose no long-term risk. Larger untreated defects, however, can lead to problems over many years. These may include progressive enlargement of the right side of the heart, increased pressure in the lung blood vessels (pulmonary hypertension), and heart rhythm disturbances (atrial arrhythmias) later in life. In rare cases, a blood clot can cross through an untreated ASD and travel to the brain, causing a stroke. This is why appropriate follow-up is important even when a child feels completely well, and why Dr Giardini recommends closing significant defects during childhood rather than waiting until symptoms develop.
The outlook for children with an ASD is excellent. Many never need any treatment at all. Those who do undergo closure, whether by catheter device or surgery, can expect to live completely normal, active lives with no restrictions. The long-term results of ASD closure in childhood are very well established, and the large majority of children require no further cardiac intervention after successful treatment.
A key part of specialist care is helping you understand exactly where your child falls on the spectrum, whether they belong to the group that simply needs periodic monitoring or the group that would benefit from closure, and when that decision should be made. If you have any questions about your child's diagnosis or would like to arrange an assessment, please do not hesitate to contact Dr Giardini's team to book an appointment.
A "hole in the heart" usually refers to an atrial septal defect, a gap in the wall between the two upper chambers. It is one of the most common congenital heart conditions and is present from birth.
Most ASDs are not dangerous. Small defects often close on their own and cause no problems. Larger defects may need treatment to prevent long-term strain on the heart, but with appropriate care the outlook is excellent.
Many children do not need any intervention at all. When treatment is needed, most secundum ASDs can be closed with a catheter-based (keyhole) procedure that avoids open-heart surgery entirely.
A patent foramen ovale (PFO) is a small opening between the atria that is normal before birth and usually closes naturally afterwards. A true ASD is a defect in the atrial septum that persists and may require monitoring or treatment.
Yes. Many small secundum ASDs close spontaneously during childhood. Dr Giardini will monitor your child with periodic echocardiograms to track whether this is happening.
When closure is needed, it is typically planned between the ages of three and six. This allows time to see if the defect closes naturally while still treating it early enough to prevent any long-term effects on the heart.
A small device is inserted through a vein in the leg and guided to the heart, where it is positioned across the hole to seal it. The procedure is performed under general anaesthetic, usually takes about an hour, and most children go home the next day.
Most children can return to normal activities within a few days of catheter closure. After surgical closure, recovery takes around six weeks. Once fully healed, there are usually no long-term activity restrictions.
Yes. Dr Giardini will arrange follow-up appointments with echocardiograms to confirm the defect is fully closed and the heart is functioning normally. Long-term follow-up requirements are usually minimal.
Most children with a small ASD or a successfully closed ASD can participate fully in sport and physical activity without any restrictions. Dr Giardini will advise you on this based on your child's individual situation.
Author: Dr. Alessandro Giardini, MD, PhD
Written 10/10/2025