
Dr. Alessandro Giardini
Most children with high cholesterol feel completely well. There are no obvious symptoms, no warning signs, and nothing to suggest a problem. Yet in some children, particularly those with familial hypercholesterolaemia (FH), cholesterol levels are elevated from birth and can cause significant damage to the arteries over decades if not identified and treated early.
This is precisely what makes high cholesterol in children both easy to miss and important to find. This page explains the condition clearly: what different forms of high cholesterol look like in childhood, why it matters, how children are identified, and what treatment involves. Dr. Alessandro Giardini sees children with inherited cardiac conditions, including FH, as part of his specialist practice in London.
Cholesterol is a fatty substance produced naturally by the body and obtained from food. The body needs a certain amount of cholesterol to build cell membranes, produce hormones, and support normal function. The problem arises when levels become too high.
There are several related terms parents encounter, and it is worth understanding what each one means.
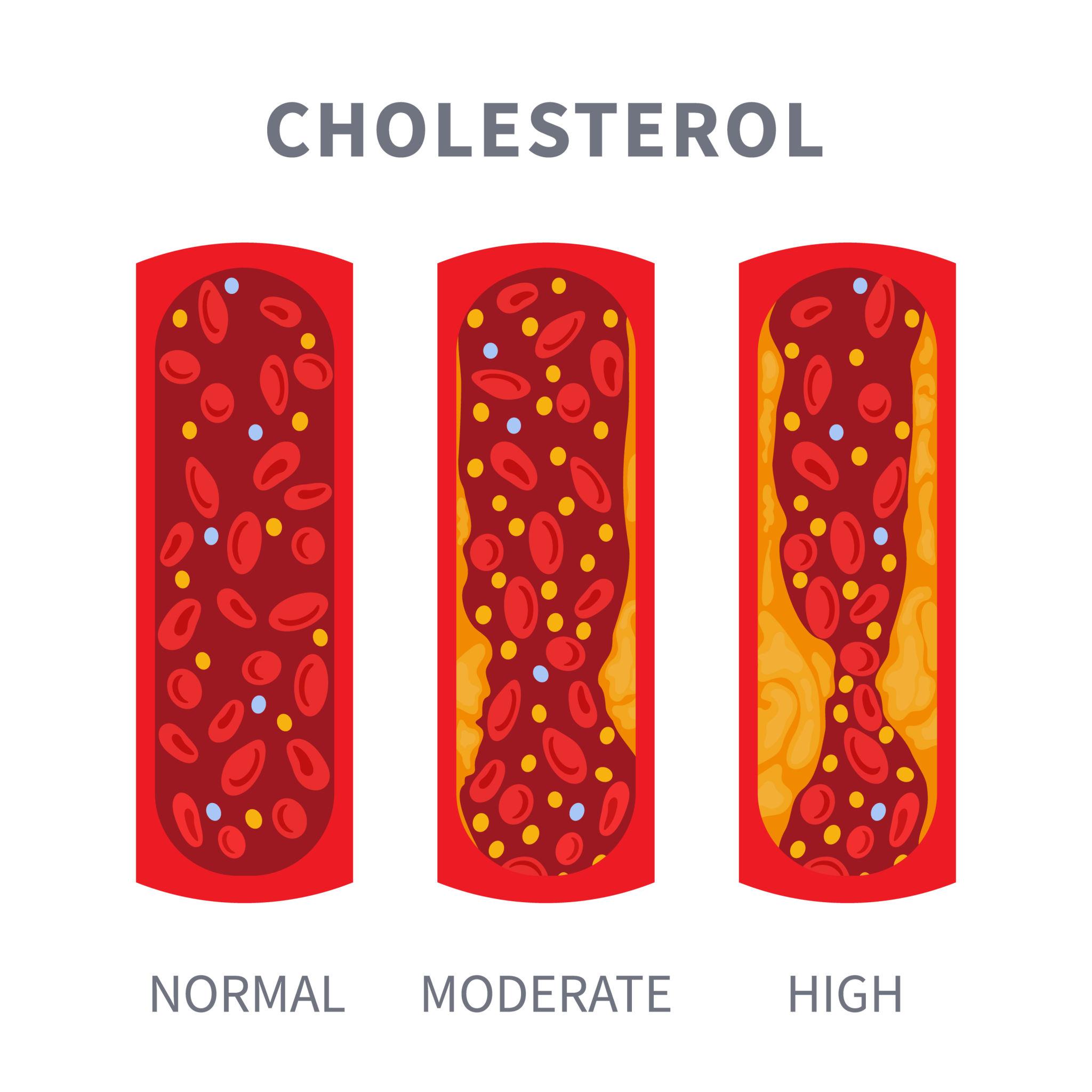
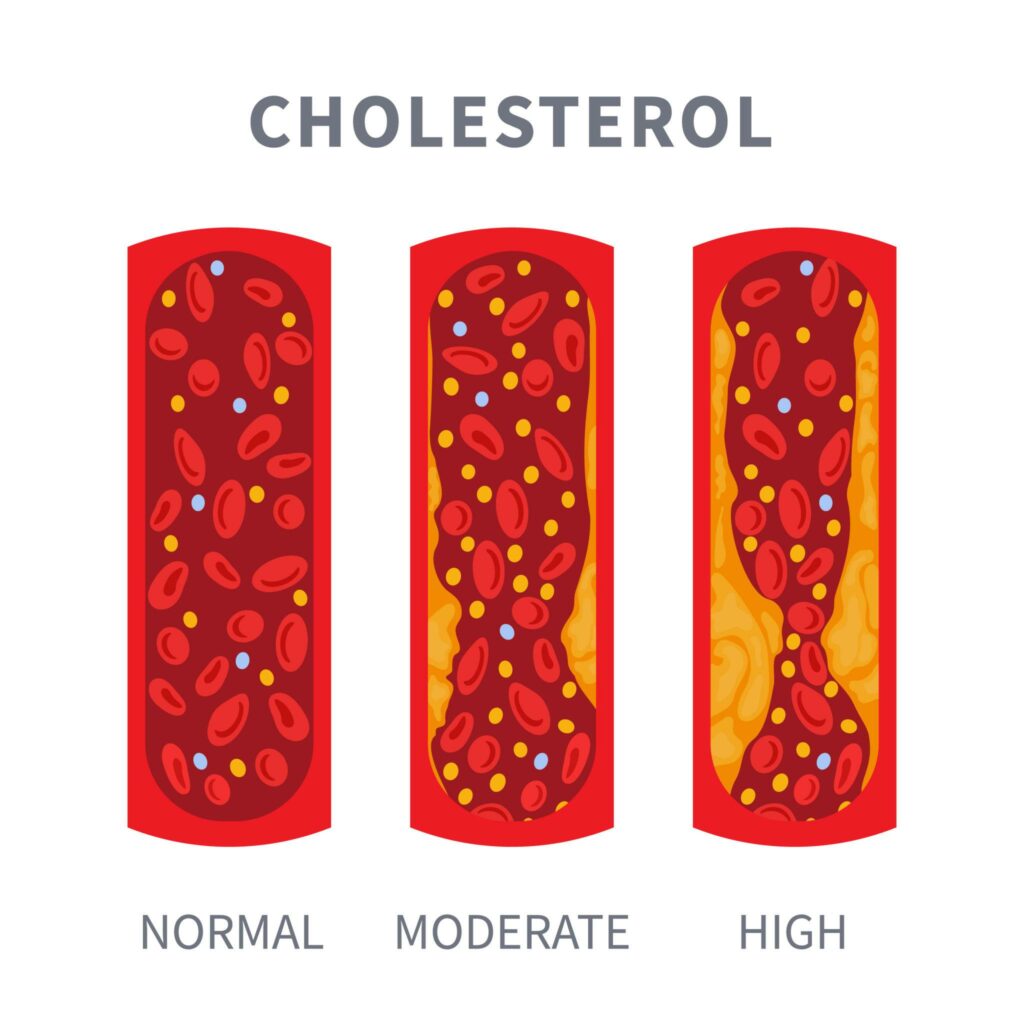
Hypercholesterolaemia refers specifically to elevated levels of cholesterol in the blood, particularly LDL cholesterol (low-density lipoprotein), often called "bad cholesterol." LDL cholesterol deposits in artery walls and contributes to atherosclerosis (narrowing and hardening of the arteries) over time. For a guide to interpreting your child's cholesterol results, see our page on normal cholesterol levels in children.
Hyperlipidaemia is a broader term covering elevated levels of any blood fats, including cholesterol and triglycerides. A child may have elevated cholesterol, elevated triglycerides, or both. Some children have a pattern of elevated triglycerides with low HDL (high-density lipoprotein or "good cholesterol"), which carries its own cardiovascular risk.
Familial hypercholesterolaemia (FH) is an inherited genetic condition in which the liver cannot clear LDL cholesterol from the blood normally. In people with FH, LDL cholesterol is elevated from birth, not because of diet or lifestyle but because of how the body processes it genetically. This is distinct from lifestyle-related high cholesterol and carries a significantly higher long-term cardiovascular risk if untreated.
This is one of the most important questions, and one that many parents find counterintuitive.
Cholesterol does not cause symptoms in children. A child with even markedly elevated LDL will feel entirely well, have normal energy, and appear healthy in every respect. Yet the damage that elevated LDL causes to artery walls begins in childhood. Fatty streaks (early atherosclerotic lesions) develop in the arteries during the teenage years in people with FH, and by early adulthood the arterial changes can be significant.

Without treatment, men with heterozygous FH experience heart attacks on average in their forties. Women with heterozygous FH experience them in their fifties. With early diagnosis and effective treatment from childhood, the risk of premature heart disease is dramatically reduced, and life expectancy can normalise.
The principle is simple: the earlier the treatment starts, the fewer years of arterial exposure to high LDL, and the lower the lifetime cardiovascular risk. This is why identifying FH in childhood genuinely saves lives.
The most common cause of mildly elevated cholesterol in children is lifestyle: a diet high in saturated fats, insufficient physical activity, and excess body weight. These children typically have moderately elevated total cholesterol and LDL, and levels often improve substantially with dietary change and increased activity. Most do not need medication.
FH is caused by a mutation (a change) in one of four well-studied genes: most commonly LDLR (the gene encoding the LDL receptor), and less commonly APOB, PCSK9, or LDLRAP1. These mutations impair the liver's ability to remove LDL cholesterol from the blood, resulting in persistently elevated LDL that does not respond adequately to lifestyle changes alone.
FH affects approximately one in every 250 people, making it one of the most common inherited conditions in the UK. Around 270,000 people in the UK have FH, yet only 15 to 17 per cent currently have a diagnosis. The vast majority are undetected.
Most people with FH have heterozygous FH (HeFH), meaning they inherited the faulty gene from one parent. If one parent has FH, each child has a 50 per cent chance of inheriting it.
A much rarer and more severe form, homozygous FH (HoFH), occurs when a child inherits faulty genes from both parents. HoFH affects approximately one in 250,000 people. LDL levels in affected children can exceed 13 mmol/L, and untreated HoFH causes heart attacks in childhood. Management of HoFH is highly specialised and requires a dedicated FH centre.
Not all high cholesterol in children is either lifestyle-related or due to FH. Secondary causes are an important group and always warrant exclusion before a primary diagnosis is made. Secondary causes include hypothyroidism (an underactive thyroid gland), diabetes mellitus, nephrotic syndrome (a kidney condition causing protein loss), cholestatic liver disease, and certain medications. A thorough clinical workup excludes these conditions, as treating the underlying cause in these children may normalise cholesterol without requiring lipid-lowering therapy.
In most children, there are none. This is perhaps the most important message for parents: high cholesterol is a silent condition. A child with FH and a markedly elevated LDL of, say, 7 mmol/L may feel entirely well, perform normally at school, and have no complaints whatsoever.
In more severe or longstanding cases, particularly in children with HoFH or severe HeFH, certain physical signs may appear. Xanthomas are yellowish, firm deposits of cholesterol that form in tendons, particularly around the Achilles tendon, the back of the hands, and the elbows. Xanthelasmas are similar yellowish deposits around the eyes. A corneal arcus (a pale ring around the iris of the eye) may also be present. These physical signs, when present in a child or young person, are strong indicators of significant FH and warrant urgent specialist referral.
FH is far more common than most parents realise, affecting approximately one in 250 people. In the UK this means around 270,000 individuals have the condition, though most remain undiagnosed. In terms of prevalence, FH is more common than many inherited conditions that receive considerably more public attention.
HoFH is rare, affecting around one in 250,000, but causes severe disease from very early in life.
In the UK, universal population screening for FH in children is not currently recommended. Instead, the UK follows a cascade testing model: when FH is diagnosed in an adult (usually a parent or other relative), their first-degree relatives (children, siblings, and parents) and second-degree relatives (aunts, uncles, grandparents, grandchildren) are offered testing.
For children not covered by cascade testing, universal cholesterol screening is recommended between the ages of nine and eleven years, with a further screen between seventeen and twenty-one years (in the US the American Academy of Paediatrics recommends this; in UK practice the approach varies and is most consistently applied in children with family risk factors).
Children should have cholesterol testing earlier than the standard ages if there is a family history of FH, if a parent or close relative has had a heart attack or stroke at a young age (under 55 in men, under 65 in women), or if a parent has been diagnosed with FH. In these higher-risk children, testing from the age of two years may be appropriate.
If a parent has been confirmed to have FH, their children should have a full fasting lipid profile and, if the LDL is significantly elevated, genetic testing. This cascade approach is the most effective way of finding undiagnosed FH early.
Diagnosis combines several elements: the LDL cholesterol level on a fasting lipid profile, the family history (particularly early heart disease in relatives), physical examination findings (tendon xanthomas if present), and genetic testing.
Children with HeFH typically have LDL cholesterol levels above 3.5 to 4 mmol/L. Children with HoFH may have LDL above 10 mmol/L even in early childhood. The target LDL in children without FH is below 2.85 mmol/L; children with FH typically have levels well above this.
Genetic testing confirms the diagnosis in the majority of cases and is important because it allows cascade testing of relatives with greater certainty. A genetic diagnosis also aids long-term management planning and, increasingly, access to newer therapies.
Lipoprotein(a), or Lp(a), is an additional inherited lipid particle that raises cardiovascular risk independently of LDL. Children with elevated Lp(a) alongside FH carry a particularly high long-term risk and may need more aggressive management. Measuring Lp(a) forms part of a comprehensive lipid assessment in children with FH or a strong family history.
Yes, and this is one of the most important practical steps after any FH diagnosis.
If a child receives a diagnosis of FH, both parents should have a lipid profile and genetic testing. If either parent has FH (which is likely), their siblings and parents should also be tested. If a parent is confirmed to have FH, all their children should be tested. This cascade testing process can identify multiple affected family members from a single index case and is the most cost-effective way of expanding FH diagnosis across the population.
For all children with elevated cholesterol, regardless of cause, dietary and lifestyle changes form the foundation of management. A diet low in saturated fat, with emphasis on fruits, vegetables, whole grains, oily fish, and unsaturated fats, helps reduce LDL cholesterol. Regular physical activity, maintaining a healthy weight, and avoiding smoking (relevant from adolescence) reduce cardiovascular risk beyond their effect on cholesterol alone.
For children with lifestyle-related mild hypercholesterolaemia, these measures may be sufficient to normalise or significantly improve cholesterol levels. For children with FH, lifestyle changes help but almost always prove insufficient on their own.
Dr. Giardini works alongside several specialist dieticians to help families adjust their diet to reap the maximum improvement from diet changes.
Statins are the main treatment for FH in children. Statins block the liver's production of cholesterol and upregulate LDL receptors, reducing LDL cholesterol by 30 to 50 per cent in most patients. Statins are safe for use in children and have an extensive evidence base in paediatric FH. In the UK, treatment typically starts from around age ten, and in children with a family history of very early cardiovascular disease, specialist guidance may support starting from age eight.
Current UK guidance targets a 50 per cent reduction in LDL cholesterol from baseline. Atorvastatin is the most commonly used statin in children in the UK.
Ezetimibe, a drug that reduces cholesterol absorption from the gut, can be added when statins alone do not achieve the target LDL reduction. Ezetimibe is well tolerated and effective as an add-on therapy.
PCSK9 inhibitors (alirocumab and evolocumab) are injectable antibodies that dramatically reduce LDL by blocking the PCSK9 protein that normally degrades LDL receptors. They are now available for adolescents in certain clinical situations and produce LDL reductions of around 50 per cent on top of statins. They are initiated through specialist services.
Evinacumab, a newer injectable therapy, received NICE approval in 2024 for treating HoFH in people aged twelve and over whose LDL is not sufficiently controlled with other therapies. It represents a significant advance for a condition that was previously extremely difficult to manage medically.
For the most severe cases of HoFH, LDL apheresis (a procedure that filters LDL from the blood, similar in principle to dialysis) may be required.
Children on statins need regular review: a full fasting lipid profile at six to twelve months in the first year of treatment and then annually, alongside liver function tests and attention to any muscle-related symptoms. Growth and general development form part of the annual review. For most children, statins are very well tolerated.
For children with mild, lifestyle-related hypercholesterolaemia, the outlook with appropriate dietary changes is generally very good, and many will have normal cholesterol levels as adults.
For children with FH, the outlook depends critically on how early the diagnosis is made and treatment started. Children who start statin treatment in childhood and maintain it throughout their lives have dramatically lower cardiovascular risk than those who remain untreated into adulthood. Studies show that early treatment can normalise life expectancy in people with HeFH. With appropriate management, the vast majority of children with FH grow up to lead normal, active lives without early heart disease.
HoFH carries a more serious prognosis without intensive treatment, but the expanding armamentarium of treatments, including PCSK9 inhibitors and evinacumab, has transformed the outlook for even these children over the past decade.
Specialist review is appropriate when a child has persistently elevated LDL cholesterol, when FH is suspected or confirmed, when cholesterol levels remain elevated despite lifestyle changes and initial treatment, when there is a family history of FH or early cardiovascular disease, or when a parent has been diagnosed with FH and their children need systematic assessment.
Dr. Alessandro Giardini provides cardiac assessments for children with high cholesterol and suspected or confirmed familial hypercholesterolaemia.
FH is an inherited genetic condition in which the liver cannot remove LDL ("bad") cholesterol from the blood normally, causing persistently elevated LDL from birth. It affects approximately one in 250 people, making it one of the most common inherited conditions in the UK. Despite this, most people with FH remain undiagnosed.
Not immediately, but it affects long-term health significantly. High cholesterol does not cause symptoms in children. Over years and decades, however, elevated LDL cholesterol damages artery walls and increases the risk of heart attack and stroke in early adulthood. Early diagnosis and treatment in childhood dramatically reduces this risk.
Not necessarily. There are several reasons a child might have elevated cholesterol, including lifestyle factors and secondary causes such as an underactive thyroid. A specialist assessment helps distinguish between these causes and identify the small proportion of children who have FH and need long-term treatment.
For children with a family history of FH or early heart disease in relatives, testing from age two is appropriate. For children without a known family risk, screening between nine and eleven years, and again between seventeen and twenty-one years, is generally recommended. If a parent has been diagnosed with FH, their children should have a lipid profile arranged promptly.
Most children with FH will need medication, typically a statin, from around the age of ten. Lifestyle changes are important but cannot adequately control LDL in FH on their own. The goal of treatment is to reduce LDL by at least 50 per cent from baseline to lower the lifetime risk of heart disease.
Yes. Statins have an extensive evidence base in children and teenagers with FH and are well tolerated. Regular monitoring of liver function and muscle symptoms forms part of routine follow-up on treatment. Side effects are uncommon, and serious adverse effects are rare.
Yes. If a child has FH, both parents and all siblings should have a lipid profile. If a parent is confirmed to have FH, extended family testing (cascade testing) is strongly recommended. This simple blood test can identify affected relatives who would otherwise remain undiagnosed until a cardiovascular event.
FH cannot be cured, as it is a genetic condition. However, its cardiovascular consequences can be prevented or substantially reduced with early diagnosis and effective treatment. Children who start statin therapy in childhood and continue it into adult life can expect a near-normal cardiovascular risk profile and normal life expectancy.
High cholesterol causes no symptoms in children. That is precisely what makes it important to identify through testing rather than waiting for symptoms. The arterial damage caused by FH builds silently over years, and by the time symptoms appear, significant disease may already be present. Early treatment prevents this damage from accumulating.
A specialist review is helpful when cholesterol levels are significantly elevated, when FH is suspected or confirmed, when a family history suggests inherited cardiovascular risk, or when you want a comprehensive risk assessment for your child. Dr. Giardini offers specialist assessments at his London clinics and welcomes referrals from GPs, paediatricians, and families directly.