Mechanisms of action, side effects & evidence-based treatment — a clinical reference for healthcare professionals
Keywords: PoTS treatment children · POTS medication paediatric · postural tachycardia syndrome drugs · dysautonomia treatment adolescents · fludrocortisone PoTS · ivabradine PoTS children · beta-blockers POTS
What is Postural Tachycardia Syndrome (PoTS) in Children?
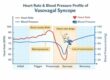
Postural Tachycardia Syndrome (PoTS) — also written as POTS — is a form of autonomic dysfunction (dysautonomia) characterised by an abnormal rise in heart rate when moving from lying to standing. In children and adolescents, the diagnostic threshold is a heart rate increase of ≥40 beats per minute (bpm) within 10 minutes of standing, with symptoms but without orthostatic hypotension (a drop in blood pressure).
PoTS most commonly begins in early-to-mid adolescence, with a female predominance. Symptoms include palpitations, lightheadedness, pre-syncope (near-fainting), chronic fatigue, headache, nausea, and cognitive impairment (‘brain fog’). These can significantly impair school attendance, physical activity, and quality of life. PoTS in children may be triggered by rapid growth, viral illness (including post-COVID PoTS), or occur alongside hypermobile Ehlers-Danlos Syndrome (hEDS) and related connective tissue disorders.
Management is multimodal. Non-pharmacological strategies — including increased fluid and salt intake (2.5 – 3.5 litres of water and 3–5 g salt daily), compression garments, and graded exercise therapy — are the foundation of treatment. Medications are added when these measures are insufficient. The following sections address each drug used to treat PoTS in children: what it does, how it works, its side effects, and the clinical evidence supporting its use.
1. Fludrocortisone for PoTS in Children
How Does Fludrocortisone Work in PoTS?
Fludrocortisone is one of the most commonly prescribed medications for postural tachycardia syndrome in children. It works by mimicking the hormone aldosterone, acting on mineralocorticoid receptors in the kidneys to increase sodium and water reabsorption. This expands blood volume, improves venous return to the heart when a child stands up, and reduces the heart’s need to compensate with excessive rate increases.
In simple terms: fludrocortisone makes the kidneys retain more fluid, increasing blood volume so the heart doesn’t have to beat as fast to maintain circulation on standing. It may also enhance the sensitivity of blood vessel receptors to adrenaline, helping to improve vascular tone.
Side Effects of Fludrocortisone
- Low potassium (hypokalaemia) — the most common electrolyte side effect; potassium levels should be monitored
- Fluid retention and ankle swelling (oedema)
- High blood pressure (hypertension), especially at higher doses
- Headaches, which may be significant
- Weight gain with prolonged use
- Suppression of adrenal gland function at higher doses
What Does the Evidence Say?
2. Beta-Blockers for PoTS in Children (Propranolol, Metoprolol)
How Do Beta-Blockers Work in PoTS?
Beta-blockers are among the most studied medications for postural tachycardia syndrome. They work by blocking beta-adrenergic receptors — the receptors that respond to adrenaline (epinephrine) and noradrenaline. In PoTS, the autonomic nervous system is overactive: standing triggers an exaggerated sympathetic (fight-or-flight) response that drives the heart rate up sharply. Beta-blockers blunt this response by blocking the signal at the receptor level, reducing heart rate and easing palpitations.
Low-dose propranolol is specifically recommended in PoTS, as high doses can worsen fatigue and exercise intolerance — symptoms already prominent in children with the condition. Cardioselective beta-blockers (metoprolol, atenolol) are preferred in children with asthma or reactive airway disease, as non-selective agents can cause bronchospasm.
Side Effects of Beta-Blockers in Children with PoTS
- Fatigue and reduced exercise capacity — particularly problematic as exercise is a cornerstone of PoTS rehabilitation
- Bradycardia (slow heart rate) and low blood pressure
- Bronchospasm — avoid non-selective beta-blockers in asthma
- Low mood and sleep disturbance
- Cold hands and feet (peripheral vasoconstriction)
- Worsening of ‘brain fog’ or cognitive symptoms
What Does the Evidence Say?
3. Ivabradine for PoTS in Children
How Does Ivabradine Work in PoTS?
Ivabradine is a targeted heart rate-lowering medication that works differently from beta-blockers, making it particularly valuable in postural tachycardia syndrome. It selectively blocks the ‘funny current’ (If) in the sinoatrial node — the heart’s natural pacemaker. This current drives the spontaneous firing rate of pacemaker cells; by inhibiting it, ivabradine slows the heart rate without affecting blood pressure, cardiac contractility, or conduction elsewhere in the heart.
This is a key advantage over beta-blockers: ivabradine lowers heart rate without reducing blood pressure, making it suitable for children with PoTS who are already hypotensive or who cannot tolerate beta-blockers. It does not affect the autonomic nervous system directly and does not worsen fatigue in the same way.
Side Effects of Ivabradine
- Phosphenes — visual disturbances (flickering or enhanced brightness in the visual field); a unique, class-specific side effect that is usually transient and resolves with dose reduction
- Bradycardia if overdosed or combined with other rate-limiting drugs
- Headache and dizziness
- Nausea and mild gastrointestinal symptoms
- Atrial fibrillation risk (uncommon in the paediatric PoTS population)
What Does the Evidence Say?
4. Midodrine for PoTS in Children
 Must not be taken within 4 hours of lying down
Must not be taken within 4 hours of lying downHow Does Midodrine Work in PoTS?
Midodrine addresses one of the core problems in postural tachycardia syndrome: excessive pooling of blood in the veins of the legs and abdomen when standing (orthostatic venous pooling). It is a prodrug, converted in the body to its active form, desglymidodrine, which activates alpha-1 adrenergic receptors in blood vessel walls. This causes constriction of both veins and small arteries, pushing blood back towards the heart and raising blood pressure slightly.
By reducing venous pooling, midodrine increases venous return to the heart, reducing the need for the compensatory tachycardia that defines PoTS. Unlike beta-blockers or ivabradine, midodrine does not directly slow the heart — it targets the underlying haemodynamic problem in the peripheral circulation. It is particularly useful in children whose PoTS is accompanied by low blood pressure or significant symptoms of cerebral hypoperfusion.
Side Effects of Midodrine
- Supine hypertension — the most important risk; midodrine raises blood pressure, which can become dangerously elevated if the child lies flat. Must be taken only when upright and avoided within 4 hours of bedtime
- Scalp tingling and ‘goosebumps’ (piloerection) — a benign but commonly noticed vasoconstrictive effect
- Urinary retention or urgency
- Headache
- Cold extremities and pallor
What Does the Evidence Say?
5. Pyridostigmine for PoTS in Children
How Does Pyridostigmine Work in PoTS?
Pyridostigmine is more commonly associated with myasthenia gravis, but it has an important role in treating postural tachycardia syndrome. It works by inhibiting acetylcholinesterase — the enzyme that breaks down acetylcholine, the main neurotransmitter of the parasympathetic nervous system and autonomic ganglia. By blocking its breakdown, pyridostigmine increases acetylcholine levels at nerve junctions throughout the autonomic nervous system.
In PoTS, this enhances ganglionic neurotransmission in the sympathetic pathways that control blood vessel tone in the limbs, improving vasoconstriction on standing and augmenting the baroreflex (the body’s reflex for correcting blood pressure and heart rate changes when standing). The key advantage is that pyridostigmine does not directly slow the heart rate or lower blood pressure when lying down — it specifically improves the orthostatic response by enhancing the autonomic reflex arc.
Side Effects of Pyridostigmine
- Nausea, vomiting, and abdominal cramping — the most common reason for dose reduction or discontinuation
- Diarrhoea and increased bowel activity
- Increased saliva production and sweating
- Urinary urgency
- Muscle cramps and twitching (fasciculations)
- Bradycardia at higher doses
What Does the Evidence Say?
6. Desmopressin (DDAVP) for PoTS in Children
How Does Desmopressin Work in PoTS?
Desmopressin is a synthetic form of antidiuretic hormone (ADH/vasopressin) that acts on V2 receptors in the collecting ducts of the kidneys, stimulating aquaporin water channels to reabsorb free water into the bloodstream. This reduces urine output and expands plasma volume, counteracting the low blood volume (hypovolaemia) that worsens PoTS symptoms — especially in the morning when children are most depleted after overnight fluid losses.
Unlike fludrocortisone, which works continuously through sodium retention, desmopressin acts more acutely and is often used on an as-needed basis — for example, before school, before prolonged standing, or at night to prevent morning hypovolaemia. It is frequently used as an adjunct rather than a primary treatment.
Side Effects of Desmopressin
- Hyponatraemia (low sodium / water intoxication) — the most serious risk, especially in children with high fluid intake; serum sodium must be monitored
- Headache
- Nausea and abdominal discomfort
- Facial flushing
- Hypertension (uncommon at doses used in PoTS)
What Does the Evidence Say?
Frequently Asked Questions: PoTS Treatment in Children
What is the best medication for PoTS in children?
There is no single best medication for postural tachycardia syndrome in children. Treatment is individualised based on the child’s predominant symptoms and underlying mechanism. Fludrocortisone and low-dose beta-blockers (especially propranolol) are most commonly used first. Ivabradine is increasingly preferred where beta-blockers cause fatigue or are contraindicated. Midodrine is used when low blood pressure and venous pooling are prominent features.
Can PoTS in children be treated without medication?
Yes. Non-pharmacological management — high fluid and salt intake, compression garments, elevating the head of the bed, graded aerobic exercise, and avoiding triggers such as prolonged standing and heat — is the first-line treatment and is effective for many children. Medications are added when these strategies alone are insufficient. Most children with PoTS improve over time with consistent non-pharmacological management.
Is PoTS in children the same as in adults?
The diagnostic criteria differ slightly: the threshold for heart rate increase is ≥40 bpm in children and adolescents (under 19 years), compared with ≥30 bpm in adults. The underlying mechanisms, medications used, and general management principles are broadly similar. Children tend to show greater spontaneous improvement over time than adults, particularly those who develop PoTS during adolescent growth spurts.
Does post-COVID cause PoTS in children?
Yes. Post-COVID PoTS has been documented in children and adolescents following SARS-CoV-2 infection, as part of Long COVID syndrome. It is thought to arise from immune-mediated autonomic nerve damage, autoantibodies against adrenergic receptors, or microvascular injury. The treatment approach is the same as for other forms of paediatric PoTS.
How long does PoTS treatment last in children?
The duration of pharmacological treatment varies. Many adolescents with PoTS experience significant improvement or full resolution by their mid-twenties as autonomic maturation completes. Treatment is typically reviewed every 6–12 months, with gradual medication tapering attempted once sustained symptomatic control is achieved alongside a consistent exercise rehabilitation programme.
Summary: Pharmacological Treatment of PoTS in Children
Postural tachycardia syndrome in children and adolescents requires a structured, individualised treatment approach. The six main drug classes used are: fludrocortisone (volume expansion via sodium retention), beta-blockers (sympathetic rate suppression), ivabradine (selective sinus node slowing), midodrine (peripheral vasoconstriction), pyridostigmine (enhanced ganglionic cholinergic tone), and desmopressin (acute volume expansion via water retention).
The evidence base in the paediatric population remains predominantly observational and extrapolated from adult randomised controlled trials. Non-pharmacological management is central and should be maintained throughout. All pharmacological treatments require careful dose titration, regular monitoring, and ongoing reassessment of both efficacy and side effects.
Key References
- Barzilai M, et al. (2020). Ivabradine treatment of postural tachycardia syndrome in young patients. Cardiology in the Young.
- Boris JR, et al. (2012). Headache in a referral population for syncope and dysautonomia. Cardiology in the Young.
- Coffin ST, et al. (2012). Desmopressin acutely decreases tachycardia and improves symptoms in the postural tachycardia syndrome. Heart Rhythm.
- Fischer PR, et al. (2012). Treatment of children with orthostatic intolerance. Clinical Pediatrics.
- Kizilbash SJ, et al. (2014). Adolescent fatigue, POTS, and recovery: a guide for clinicians. Pediatric Clinics of North America.
- Low PA, et al. (1997). Efficacy of midodrine vs placebo in neurogenic orthostatic hypotension. JAMA.
- Raj SR, et al. (2005). The postural tachycardia syndrome (POTS): pathophysiology, diagnosis & management. Circulation.
- Raj SR, et al. (2005). Acetylcholinesterase inhibition improves tachycardia in postural tachycardia syndrome. JAMA.
- Raj SR, et al. (2009). Propranolol decreases tachycardia and improves symptoms in the postural tachycardia syndrome. Circulation.
- Ruzieh M, et al. (2017). Ivabradine in the treatment of postural tachycardia syndrome. Annals of Noninvasive Electrocardiology.
- Salim MA & Di Sessa TG (2005). Effectiveness of fludrocortisone and salt in preventing syncope recurrence in children. Journal of the American College of Cardiology.
- Stewart JM (2002). Pooling in chronic orthostatic intolerance. Journal of Pediatrics.
- Taub PR, et al. (2012). Beneficial effects of ivabradine in patients with inappropriate sinus tachycardia. Annals of Noninvasive Electrocardiology.