
Dr. Alessandro Giardini
Being told that your child has a bicuspid aortic valve (BAV) can feel unexpected, particularly when it is found during a routine scan or while investigating a heart murmur. The most important thing to understand from the outset is that most children with a bicuspid aortic valve grow up completely well, with no symptoms and no limitations on their daily life.
BAV is the most common congenital heart condition. In most children it does not require treatment, it simply needs sensible monitoring over time. This page explains clearly what BAV is, what it means for your child's health and activity levels, and when, if ever, intervention may be needed.
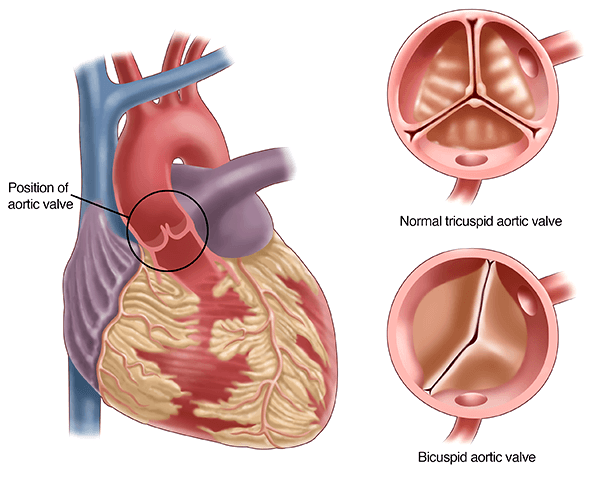
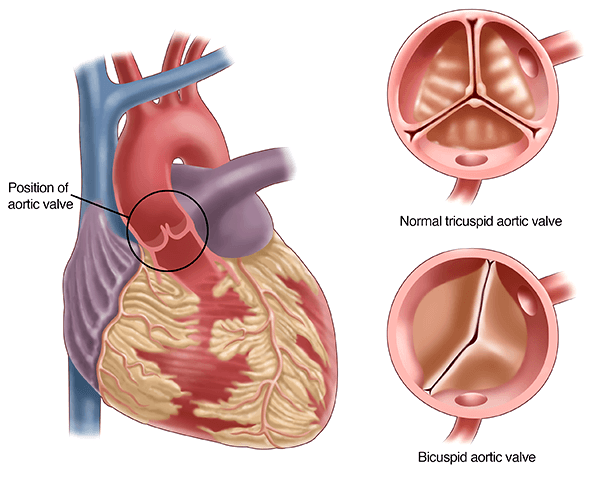
The aortic valve sits between the heart and the aorta, the large artery that carries blood from the heart to the rest of the body. Its job is to open fully when the heart pumps and close completely between beats, ensuring blood flows in one direction only.
In most people, the aortic valve has three leaflets (flaps). This three-leaflet design, known as a tricuspid valve, opens symmetrically and manages the forces of blood flow very efficiently. In a bicuspid aortic valve, two of the three leaflets fuse together during foetal development, leaving the valve with only two leaflets instead of three. The valve still opens and closes, and in most children it does so perfectly well. Its two-leaflet structure does mean that over a lifetime it may face slightly different mechanical stresses than a normal tricuspid valve.
BAV is not an acquired disease and not something that develops because of anything that happened during pregnancy. The valve simply forms this way, and that variation is a remarkably common one.
BAV is the most prevalent congenital heart defect in children and adults, affecting between 0.5 and 1 per cent of the general population. Millions of people worldwide have a bicuspid aortic valve. The vast majority live normal, active lives without ever needing intervention.
BAV can occur on its own or occasionally in association with other conditions, including narrowing of the aorta (coarctation), and is also more commonly seen in girls with Turner syndrome. In most children, it is an isolated finding.
In most children, a bicuspid aortic valve functions normally or very nearly normally, and the heart performs exactly as it should. The primary reason we follow children with BAV over time is that, in some individuals, the valve or the aorta may develop changes gradually as the child grows. The three main developments that can occur are:
Aortic stenosis occurs when the valve narrows and does not open fully, making the heart work harder to push blood through it. Aortic regurgitation develops when the valve does not close completely, allowing a small amount of blood to leak back into the heart after each beat. Aortic dilatation means the main artery leaving the heart gradually enlarges. This happens because the altered blood flow pattern through a bicuspid valve places different mechanical stresses on the aortic wall, and because some of the genetic factors behind the bicuspid anatomy also affect the aortic wall's structure.
Regular echocardiographic follow-up detects these changes early. In the great majority of children they either do not develop during childhood or remain mild and stable. Only around 12 to 15 per cent of children with BAV require any form of intervention before adulthood.
Most children with BAV have no symptoms at all. This is not a condition that typically announces itself through discomfort or reduced energy in childhood. Most children feel entirely well and function normally.
When symptoms do occur, they are more common in adolescence than in younger children. They tend to reflect significant valve narrowing or leakage rather than the bicuspid anatomy itself. Symptoms that may indicate the valve is becoming significantly affected include reduced exercise tolerance, unusually easy fatigue during physical activity, chest discomfort on exertion, breathlessness, and, less commonly, dizziness or lightheadedness. Fainting during exertion in a child with known BAV should always prompt specialist review.
Parents should not interpret their child feeling entirely well as meaning that follow-up is unnecessary. The absence of symptoms is the expected situation in childhood. Monitoring matters precisely because it detects gradual changes before symptoms develop.
The standard investigation is an echocardiogram, an ultrasound scan of the heart. It visualises the valve structure, assesses how well it opens and closes, quantifies any stenosis or regurgitation, and measures the dimensions of the aorta. The scan is painless, involves no radiation, and takes around 30 to 45 minutes.
One of the characteristic findings on clinical examination is an ejection click, a brief, sharp sound heard with the stethoscope at the moment the bicuspid valve opens. This click, sometimes accompanied by a soft heart murmur, is often the first clue that prompts referral for echocardiography. Not all children with BAV have an audible click, but when present it is a distinctive sign that an experienced paediatric cardiologist will recognise.
BAV is most commonly detected in one of three ways: when a doctor hears a murmur during a routine examination and refers for echocardiography; when it is found incidentally during a scan performed for another reason; or through family screening, when a parent or sibling has already been diagnosed.
In older children and adolescents where the aorta appears enlarged on echocardiogram, cardiac MRI may be arranged for a more precise assessment of aortic dimensions, as it gives a more comprehensive view of the entire aorta without radiation exposure.
In younger children who are unable to lie still for the duration of an MRI scan without general anaesthetic, a cardiac CT can provide an alternative means of assessing the aorta in detail. CT is faster and does not require sedation in most cases, although it does involve a small dose of ionising radiation. The choice between MRI and CT is made on a case-by-case basis depending on the child's age, the clinical question being asked, and whether anaesthesia can be avoided.
The majority of children with BAV do not need medication, do not need surgery, and do not need any restriction on activity. The focus is entirely on monitoring over time, to ensure that any changes to valve function or aortic size are detected early and managed appropriately if they occur.
In children where the aorta is showing early signs of enlargement but has not reached the threshold for surgical intervention, medication may be considered. Beta-blockers and, in some cases, angiotensin receptor blockers can help reduce the rate of aortic dilatation by lowering the mechanical stress on the aortic wall with each heartbeat. These medications are well tolerated and are used as a precautionary measure to delay or prevent the need for surgery. Dr Giardini will discuss whether medical treatment is appropriate based on your child's individual aortic measurements and rate of change over time.
Treatment is only needed if the valve or aorta becomes significantly affected. The main indications are moderate to severe aortic stenosis, significant aortic regurgitation causing the heart to enlarge, or progressive dilatation of the aorta beyond safe thresholds.
When intervention is needed, the options depend on the child's age, the valve anatomy, and the nature of the problem. Balloon aortic valvuloplasty is a catheter-based procedure that relieves significant stenosis without open heart surgery, and surgeons often choose it first in younger children. Surgical valve repair, where the valve leaflets are reconstructed, offers growing children a better option than valve replacement wherever the anatomy allows. The Ross procedure, in which the child's own pulmonary valve replaces the aortic valve, remains an important option in specialist centres for cases where repair is not feasible. Valve replacement with a mechanical or biological prosthesis generally suits older adolescents and adults better than younger children.
Families can take reassurance that intervention in childhood is the exception rather than the rule. When it does become necessary, specialist teams with considerable experience plan and carry it out carefully.
Regular echocardiographic follow-up is the cornerstone of managing BAV in children. Review frequency is tailored to each child based on how the valve is functioning and the size of the aorta. Children with normal valve function and a normal aorta may need echocardiograms only every 2-3 years. Those with any degree of valve dysfunction or aortic enlargement are reviewed more frequently.
Follow-up appointments also give families the opportunity to discuss any new symptom, review activity advice, and raise questions that accumulate between visits. Dr. Giardini's approach in clinic is to ensure families understand exactly what is being monitored and why, and to give clear, specific advice rather than generic reassurance.
For most children with BAV, the answer is yes, without restriction. Children with normal or near-normal valve function and a normal aortic size can participate fully in all sports, including competitive sport. Physical activity is good for them, and there is no reason to limit it.
Restrictions are only considered in a minority of children, specifically those with significant aortic stenosis, significant valve leakage, or an enlarged aorta. In these situations Dr. Giardini will give specific, tailored guidance. Each child is assessed individually and the advice is based on the actual findings at echocardiography, not on the diagnosis of BAV alone.
For adolescents considering high-intensity competitive sport at elite level, a formal pre-participation cardiac assessment is often appropriate, and Dr. Giardini's experience in exercise physiology in children with heart conditions is particularly relevant in this context.
Yes. BAV has a clear genetic basis, and first-degree relatives of a child with BAV (parents and siblings) have a meaningfully higher chance of also having the condition. Current American Heart Association guidelines recommend echocardiographic screening for all first-degree family members, even those with a normal examination. Many people with BAV are entirely asymptomatic and would not otherwise know to seek assessment, which is exactly why screening matters.
Families in which BAV has been identified in a child should therefore discuss screening with their cardiologist, as identifying the condition in a parent or sibling allows appropriate monitoring to be established for them too.
The long-term outlook for children with BAV is very good. Most children grow normally, remain symptom-free throughout childhood and adolescence, and go on to live full, active adult lives. Appropriate monitoring ensures that any changes to valve function or aortic size are detected early and managed at the right time, before they cause significant problems.
Honesty requires acknowledging that BAV needs ongoing follow-up into adult life. The transition from paediatric to adult congenital cardiology services is a normal part of care for young people with BAV. It ensures continuity of monitoring as they reach adulthood.
Children with a bicuspid aortic valve have a small but recognised risk of developing endocarditis, a serious infection of the heart valve caused by bacteria entering the bloodstream. The turbulent blood flow across a bicuspid valve can make the valve tissue more susceptible to infection. Good dental hygiene, including regular brushing, flossing and routine dental check-ups, is the single most important way to reduce this risk. Current guidelines do not recommend routine antibiotics before dental procedures for most children with BAV, although this may be advised for the first six months after any valve intervention. Dr Giardini will clarify whether specific endocarditis precautions apply to your child.
A specialist review helps confirm the diagnosis clearly, assess valve function and aortic dimensions accurately, and provide specific advice about sport and physical activity. It also establishes an appropriate follow-up plan and addresses any anxiety about what the diagnosis means for daily life.
Dr. Alessandro Giardini provides expert assessment and follow-up for children and adolescents with bicuspid aortic valve across several London locations. His focus is on combining clinical rigour with clear, practical explanations that give families genuine confidence in how their child is being managed.
In most cases, no. The great majority of children with BAV are completely well and live normal lives without needing treatment. Regular monitoring is important, but the diagnosis does not mean your child is at significant risk or that intervention is likely in childhood. A consultation with a paediatric cardiologist will provide a clear picture of your individual child's situation.
Most children do not need surgery in childhood. Around 12 to 15 per cent of children with BAV require some form of intervention before adulthood, which means the large majority do not. Intervention is only needed if the valve becomes significantly narrowed or leaky, or if the aorta enlarges significantly. These changes develop slowly and regular monitoring reliably detects them.
Yes, in most cases. If the valve and aorta are functioning and sizing normally, there are no restrictions on sport, including competitive sport. Your cardiologist will advise clearly if there are any specific concerns based on your child's echocardiogram findings.
It can change over time, but progression during childhood is often slow. Many children remain entirely stable for years, and some never develop significant changes at all. Regular follow-up ensures that any changes are identified early and acted on at the right time.
Yes. Because BAV runs in families, current guidelines recommend that all first-degree relatives (parents and siblings) have a screening echocardiogram, even if they feel entirely well and have a normal heart examination. The scan is simple and painless, and specialist teams strongly recommend it.
No. The valve structure does not change. However, many bicuspid valves function normally for many years, and having a bicuspid valve does not mean that problems are inevitable. What matters clinically is how well the valve is functioning and whether any associated aortic changes are occurring.
In most cases, no. With appropriate monitoring and timely management of any valve or aortic changes that develop, children with BAV typically have a normal life expectancy. This is why long-term follow-up matters: it is precisely the tool that ensures the condition remains well managed throughout life.
The first step is a thorough echocardiographic assessment to establish clearly how the valve is functioning and what the aortic dimensions are. From that baseline, a personalised follow-up plan is put in place. Most families leave the first consultation with a clear understanding of their child's individual situation, a specific follow-up schedule, and clear advice about activity. For many, that first consultation is substantially more reassuring than they expected.
Author: Dr. Alessandro Giardini, MD, PhD
Written 03/04/2026