
Dr. Alessandro Giardini
Kawasaki disease is a condition where the body develops an inflammation of the small and medium sized arteries of the bodyy. To explain what an inflammation is, it is fair to compare it to a burn, where the area affected becomes tender, swollen, red and hot. This inflammation causes a weakening of the wall of the body arteries which can cause in children the swelling (aneurysm) of the arteries. Sometimes, the healing process can instead cause a narrowing of the arteries. The disease most commonly causes dilatation of the coronary arteries (the arteries that feed the heart itself with oxygen and nutrition) and it is the main cause of acquired heart disease in children. It is estimated that around 8 in every 100,000 children develop Kawasaki disease every year in the UK.
The disease starts as many other febrile illnesses and children present with several symptoms and signs, which are used to make the diagnosis of Kawasaki disease.
These symptoms and signs are:
Despite significant research efforts to try to understand the cause of Kawasaki disease, we still do not know the exact cause. It is believed that an infection (germ or virus) could trigger the inflammation typical of the disease.
The condition is called Kawasaki disease after the name of the first doctor (from Japan) who first described it. Children of asian and pacific origin are at higher risk of developing the condition. The conditions is also more common in children younger than 5 years of age and in boys rather than girls.
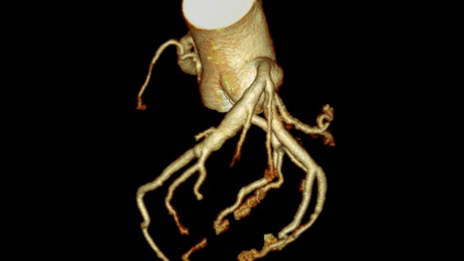
The majority of children recover from the disease as soon as the condition is suspected and appropriate treatment is delivered. Complications generally occur before appropriate treatment is initiated or when the disease goes untreated for some time and fortunately affect only a minority of children. The key in avoiding complications is early diagnosis and treatment. The most common complication is dilatation of the coronary arteries. In the majority of cases, when the coronary arteries are affected the dilatation is mild. However, the dilatation can be significant in a minority of children (giant aneurysms). In children with giant aneurysms of the coronary arteries there is the risk of blood clots forming and causing a heart attack. The inflammation can sometimes extend to other parts of the heart and to other arteries of the body causing a drop in heart function, problems with the heart rhythm (arrhythmias or fast/slow heart beats) and problems with the heart valves.
Children where the diagnosis is suspected have to be admitted to hospital for investigation and assessment by several specialists which include a general paediatrician, a paediatric cardiologist, an infection disease expert and sometimes an expert of inflammation like a rheumatologist. Children have to undergo clinical examination, blood testing for signs of inflammation and to exclude other causes of fever, a urine test, an electrocardiogram (ECG) and an echocardiogram by a paediatric cardiologist to look at the size of the coronary arteries and rule out coronary aneurysms.
Children with a suspected diagnosis of Kawasaki disease will be given intravenous immunoglobulins (antibodies which are donated by blood donors) and high dose aspirin. Some children might require a second dose of immunoglobulins or steroid administration if the have a relapse of Kawasaki disease, if they fail to respond to immunoglobulins or if they are found to have giant aneurysms. If the first echocardiogram does not show any coronary artery problem then children would receive aspirin for a short period of time. A follow-up echocardiogram by a paediatric cardiologist is recommended at about 3 weeks follow-up. If the coronary arteries are affected then children might require longer courses of aspirin or sometimes a more aggressive blood thinning treatment to avoid the creation of blood clots in the coronary arteries.
In the majority of children with Kawasaki disease the long term outlook is very good. Long term management revolves around avoiding the known risk factors for coronary artery disease like overweight, abnormal blood lipid, tobacco smoking and sedentary lifestyle.
Kawasaki disease is a condition that causes inflammation in blood vessels throughout the body. It mainly affects young children and can involve the heart, particularly the coronary arteries. With early treatment, most children recover completely.
The most important early sign is a high fever lasting more than 5 days. Other features can include red eyes, rash, red lips or tongue, swollen hands and feet, and swollen glands in the neck. Not all children have all symptoms.
The main concern is that it can affect the coronary arteries, which supply blood to the heart. If untreated, this can lead to complications. The reassuring news is that early treatment significantly reduces this risk.
In most cases, no — especially when treated early. Serious complications are uncommon with prompt medical care. The key is recognising the condition and starting treatment at the right time.
You should seek medical advice if your child has a persistent fever for more than 5 days, especially if associated with rash, red eyes, or changes in the mouth or hands. If your child seems unwell, it is always reasonable to have them assessed earlier.
There is no single test. Diagnosis is based on a combination of symptoms, examination findings, and blood tests. An echocardiogram is usually performed to assess the heart and coronary arteries.
Treatment involves intravenous immunoglobulin (IVIG) and aspirin, usually given in hospital. This treatment is very effective when started early and helps reduce inflammation and protect the heart.
Most children do not. If treatment is given early, the risk of long-term heart complications is very low. Some children need follow-up scans to monitor the coronary arteries, but the majority recover fully.
Recurrence is uncommon but can happen in a small number of children. If your child develops similar symptoms again, particularly prolonged fever, they should be reassessed.
Yes. The vast majority of children go on to live completely normal, active lives. Any long-term follow-up depends on whether the heart was affected, but most children have no lasting issues.
Author: Dr. Alessandro Giardini, MD, PhD
Written 03/04/2026