Why Does Pre-Sport Cardiac Screening Matter?
The sudden death of a young athlete is one of the most shocking and heartbreaking events imaginable. Although rare (estimated at approximately 1 in 50,000 to 1 in 80,000 young athletes per year) these deaths are often caused by previously undetected heart conditions that are, in many cases, identifiable through screening.
The vast majority of children and teenagers who engage in sport have completely healthy hearts. The goal of cardiac screening is not to frighten families or restrict children from
physical activity as exercise is one of the most beneficial things a child can do for their health. The goal is to identify the small number of children who have a heart condition that
requires assessment, guidance, or treatment before they engage in intense competitive sport.
Knowing whether your child has a normal heart before they compete at a high level is not just peace of mind. In some cases, it can be lifesaving.
Who Should Consider Pre-Sport Cardiac Screening?
While all children benefit from a healthy lifestyle and access to sport, cardiac screening is particularly relevant in certain groups:
– Children and teenagers entering competitive sport: Those who are planning to train intensively or compete at club level and above, whether in football, athletics, swimming, cycling, or any other discipline.
– Children with symptoms during exercise: Any child who experiences chest pain, breathlessness disproportionate to the level of effort, palpitations, dizziness, or fainting during or after exercise should be assessed by a cardiologist before continuing sport.
– Children with a family history of heart conditions: Particularly if a close family member has been diagnosed with an inherited cardiac condition (such as hypertrophic
cardiomyopathy, Long QT syndrome, or Brugada syndrome), or if there has been an unexplained sudden death or cardiac arrest in the family under the age of 50.
– Children diagnosed with a heart condition: Who wish to participate in competitive sport and require a formal assessment of their suitability to do so.
– Children being considered for elite or professional sport: As part of the standard medical assessment required by many sporting bodies and academies.
What Does a Pre-Sport Cardiac Screen Involve?
A comprehensive pre-sport cardiac screen typically includes:
Medical and Family History
A detailed discussion about personal symptoms, past medical history, and family history of heart conditions, sudden deaths, or unexplained fainting in young relatives. This clinical history is one of the most informative parts of any screening assessment and helps identify children who are at higher risk.
Physical Examination
A full cardiovascular examination, including listening to the heart for murmurs, checking blood pressure, and assessing for physical features that may suggest an underlying condition (such as the tall stature and joint laxity associated with Marfan syndrome, which carries a risk of aortic rupture).
Electrocardiogram (ECG)
A 12-lead ECG records the electrical activity of the heart and can detect a wide range of conditions that might not be apparent on clinical examination alone. These include:
Hypertrophic cardiomyopathy (HCM), the most common cause of sudden cardiac death in young athletes. Long QT syndrome, Wolff-Parkinson-White syndrome (WPW), Brugada syndrome, arrhythmogenic right ventricular cardiomyopathy (ARVC), short QT syndrome and other electrical and structural abnormalities.
An ECG is non-invasive, quick, and inexpensive. European cardiology guidelines (including those of the European Society of Cardiology) recommend ECG as part of pre-participation screening in competitive athletes, alongside clinical history and examination.
Echocardiogram (Heart Ultrasound)
An echocardiogram provides a real-time ultrasound image of the heart, allowing assessment of its structure and function. It is the key test for diagnosing hypertrophic cardiomyopathy,
valve abnormalities, and structural defects. Not every screening programme routinely includes an echocardiogram (it is more expensive and time-consuming than an ECG), but it is recommended for children with positive findings on ECG, clinical history, or examination, and is offered as standard in a comprehensive specialist cardiac screen.
Additional Tests if Needed
Depending on the findings, further investigations may include exercise testing (to assess the heart’s response to physical stress), Holter monitoring (24-hour heart rhythm
recording), cardiac MRI, or genetic testing.
What Conditions Can Screening Detect?
Pre-sport cardiac screening is designed to identify conditions that increase the risk of sudden cardiac arrest during intense physical activity. The most important of these are:
– Hypertrophic Cardiomyopathy (HCM): The most common cause of sudden cardiac death in young athletes. The heart muscle is abnormally thickened, which can obstruct blood flow and predispose to dangerous heart rhythms during exertion. Many affected individuals have no symptoms prior to screening.
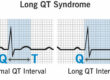
– Long QT Syndrome: An inherited condition in which an abnormality in the heart’s electrical recovery can trigger a dangerous heart rhythm called torsades de pointes, often triggered by exercise or sudden fright.
– Wolff-Parkinson-White Syndrome (WPW): An accessory electrical pathway in the heart that can, in rare cases, precipitate a dangerously rapid arrhythmia during exercise.
– Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC): A rare condition in which the heart muscle, particularly on the right side, is gradually replaced by fatty or fibrous
tissue, making the heart prone to dangerous arrhythmias, often triggered by endurance exercise.
– Brugada Syndrome: An inherited electrical condition associated with a risk of ventricular arrhythmia, though typically more at rest or during fever than during exercise.
– Marfan Syndrome and related connective tissue disorders: Can be associated with dilatation of the aorta, carrying a risk of aortic dissection or rupture during intense physical
effort.
– Anomalous coronary arteries: Abnormal origin or course of the coronary arteries can cause compression during exercise, leading to sudden cardiac death. Usually detectable on echocardiography.
What Happens If Something Is Found?
A positive finding on a cardiac screen does not necessarily mean your child cannot do sport. Many children with cardiac findings participate fully in physical activity with appropriate
monitoring and guidance. The role of the screening cardiologist is to:
1. Accurately diagnose or characterise the finding
2. Assess the level of risk it carries in the context of sport
3. Advise on what sports and intensities are safe
4. Recommend treatment if appropriate (for example, catheter ablation for WPW, or medication for Long QT syndrome)
5. Provide clear written documentation for schools, clubs, and sporting bodies
Some conditions, such as severe hypertrophic cardiomyopathy do require restriction from competitive sport. Others like successfully ablated WPW allow full, unrestricted sporting participation after treatment. Many findings are minor and require no restriction at all.
The decision is never taken lightly, and the aim is always to enable as much physical activity as safely possible, because the physical and mental health benefits of sport are enormous.
How Often Should Screening Be Repeated?
For children and teenagers who are actively competing, cardiac screening is not always a one-time event. Some inherited conditions like hypertrophic cardiomyopathy and
ARVC can progress during adolescence as the heart grows and changes. Repeat screening every 2–3 years during teenage years is often recommended for competitive
athletes.
Frequently Asked Questions
Is cardiac screening before sport mandatory in the UK? There is currently no universal mandatory cardiac screening programme for young athletes in the UK, though several
sporting bodies including Premier League football academies and some athletics programmes have their own screening requirements.
At what age should cardiac screening start?
Screening is most relevant once children begin competitive sport in earnest, which for many is around 12–14 years of age. However, it is appropriate at any age if there are symptoms, a family history of concern, or a child is entering an elite sporting programme.
Is an ECG enough, or does my child need an echocardiogram too?
An ECG is the most widely used and cost-effective single screening test. However, an echocardiogram adds valuable
information and is recommended as part of any comprehensive screen. A normal ECG does not exclude all cardiac conditions as some structural abnormalities are not
ECG-detectable.
What if I have a family history of sudden cardiac death?
This is one of the strongest indications for cardiac screening. Any unexplained sudden death or cardiac arrest in a family
member under 50 years of age warrants evaluation of first-degree relatives. The investigation will include detailed history-taking, ECG, echocardiogram, and potentially genetic testing depending on the circumstances.
Can a perfectly healthy-looking, fit child have a dangerous heart condition?
Yes, and this is precisely why screening matters. Many of the conditions that cause sudden cardiac death in young people produce no symptoms whatsoever. A fit, athletic, apparently healthy child can be affected. Screening provides an important safety net.
Does cardiac screening give a guarantee that sport is completely safe?
No test can provide an absolute guarantee of safety. However, comprehensive cardiac screening substantially reduces the risk of an undetected condition causing harm during sport. The overwhelming majority of children who are screened and found to have a normal heart can go on to train and compete with complete reassurance.
Dr Alessandro Giardini is a Consultant Paediatric Cardiologist at Great Ormond Street Hospital and a specialist in cardiac screening, exercise physiology, and
inherited cardiac conditions in children and young people. Pre-sport cardiac assessments are available at Great Ormond Street Hospital, The Portland Hospital and Chase Lodge Hospital.
Dr. Alessandro Giardini, MD, PhD
Consultant Paediatric Cardiologist, Great Ormond Street Hospital and The Portland Hospital
Written 27/03/2026