

What is an ASD?
An atrial septal defect (ASD) or a “hole in the heart” is a type of congenital heart defect in which there is an abnormal opening in the wall that normally divides the back chambers of the heart (the atria). It’s not clear why, but ASDs are more common in girls than in boys. A genetic cause of the ASD can be found in some families, but there’s no clear cause in the majority of children with an atrial septal defect. In order to understand the consequences of an ASD we have to start considering what happens in a normal heart. In the normal circulation, the blood which is low in oxygen returns to the right-sided back chamber (right atrium) and passes into the right-sided pumping chamber (known as the right ventricle) from where it is pumped to the lungs. Once the blood has been enriched in oxygen, it flows back to the left sided back chamber (left atrium) and subsequently passes into the left pumping chamber (left ventricle), from where it is then pumped into the general circulation to provide oxygen to the body. This video shows very clearly and simply what the blood flow in a normal heart is like.
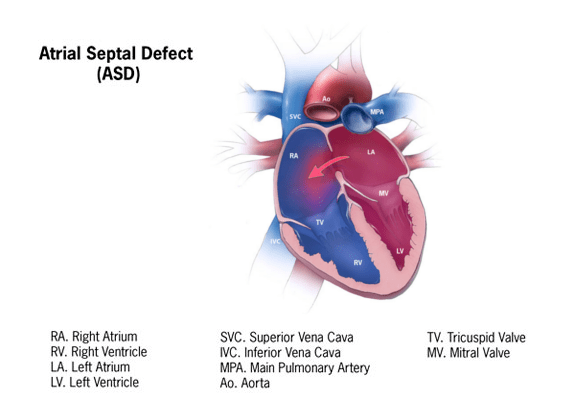
In the presence of an ASD, some of the blood that arrives in the left atrium falls through the ASD back into the right atrium and from there it is pumped again to the lungs from the right sided pumping chamber. One of the main consequences of an ASD is therefore that some of the blood that should be pumped into the general circulation is shunted across the ASD back to the lungs. As a result of this, the amount of blood that the right side of the heart is handling increases (causing swelling of the right atrium and right ventricle) as well as the blood flow to the lungs. This increased blood flow to the lungs can create a vibration as it passes through the pulmonary valve, creating a heart murmur. The amount of blood crossing the atrial hole clearly depends on the size of the ASD. A small passage between the two atria is very common in children soon after birth. This is referred to as patent foramen ovale (or PFO). Such a small hole has a specific purpose during foetal life, which is that of allowing the growth of the left side of the heart. This type of small defect invariably closes in the first 2 years of life and should largely be regarded as normal in a child in the first 6-12 months of life. Larger holes might still progress to spontaneous closure and generally
When and how to treat an ASD?
The decision of whether an ASD requires treatment and the type of treatment is based on the following factors:
- Position of the ASD: there are 4 main groups of ASD depending on its position. Centrally located ASDs (called ostium secundum) are amenable to interventional (key hole) closure if the size of the defect is not excessive both in absolute terms and in relation to the child’s heart size (remember that your child’s heart size is roughly the same as his fist). Interventional “key hole” closure is achieved by using a specifically designed double umbrella device. Additionally, it is important to establish if there is enough healthy tissue around the ASD where the device can anchor itself safely. The other types of ASD, where the defects are not centrally located in the atrial septum or where the ASD opens in proximity to other surrounding heart structures, require surgical closure of the defect.
- Size of the ASD: small ASDs are generally well tolerated and the heart does not show any sign of swelling. Larger holes allow for more blood shunting to the lungs.
- Presence of symptoms: frequent chest infection, reduced energy levels and, less often, failure to thrive. Palpitations and irregular heartbeats can be seen in older children.
- Presence of right heart swelling on the echocardiogram: as we can anticipate that an atrial septal defect which is causing right heart swelling will cause complications later in life, paediatric cardiologists often recommend closing these ASDs early in childhood.
- Age of the child: in younger children the interventional (key hole) closure of the defect can be very difficult and potentially unsafe. In some children it may be beneficial to wait to see if the child can reach a heavier weight or the ASD to become slightly smaller before attempting “key-hole” device closure. In any case the decision has to be made on an individual basis for every child.
Whether closure is achieved by key hole intervention or by open heart surgery the vast majority of ASDs are treated successfully with few or no complications.